

Current Insights into Atopic March
- PMID: 34828780
- PMCID: PMC8620020
- DOI: 10.3390/children8111067
Current Insights into Atopic March
Abstract
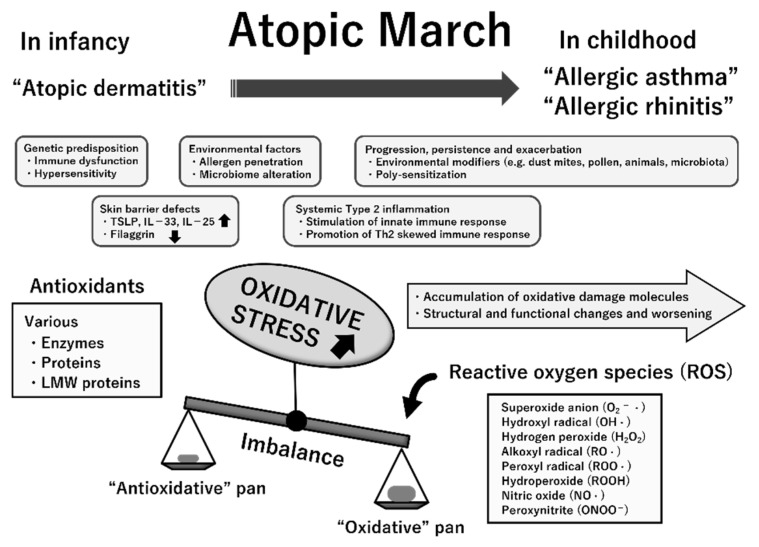
The incidence of allergic diseases is increasing, and research on their epidemiology, pathophysiology, and the prevention of onset is urgently needed. The onset of allergic disease begins in infancy with atopic dermatitis and food allergy and develops into allergic asthma and allergic rhinitis in childhood; the process is defined as "atopic march". Atopic march is caused by multiple immunological pathways, including allergen exposure, environmental pollutants, skin barrier dysfunction, type 2 inflammation, and oxidative stress, which promote the progression of atopic march. Using recent evidence, herein, we explain the involvement of allergic inflammatory conditions and oxidative stress in the process of atopic march, its epidemiology, and methods for prevention of onset.
Keywords: alarmin; allergic asthma; allergic rhinitis; atopic dermatitis; atopic march; early intervention; emollient; epidemiology; food allergy; group 2 innate lymphoid cells; oxidative stress; phenotype; skin barrier dysfunction; specific biomarker; type 2 inflammation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
