

The Impacts of Aspergillosis on Outcome, Burden and Risks for Mortality in Influenza Patients with Critical Illness
- PMID: 34829211
- PMCID: PMC8620692
- DOI: 10.3390/jof7110922
The Impacts of Aspergillosis on Outcome, Burden and Risks for Mortality in Influenza Patients with Critical Illness
Abstract
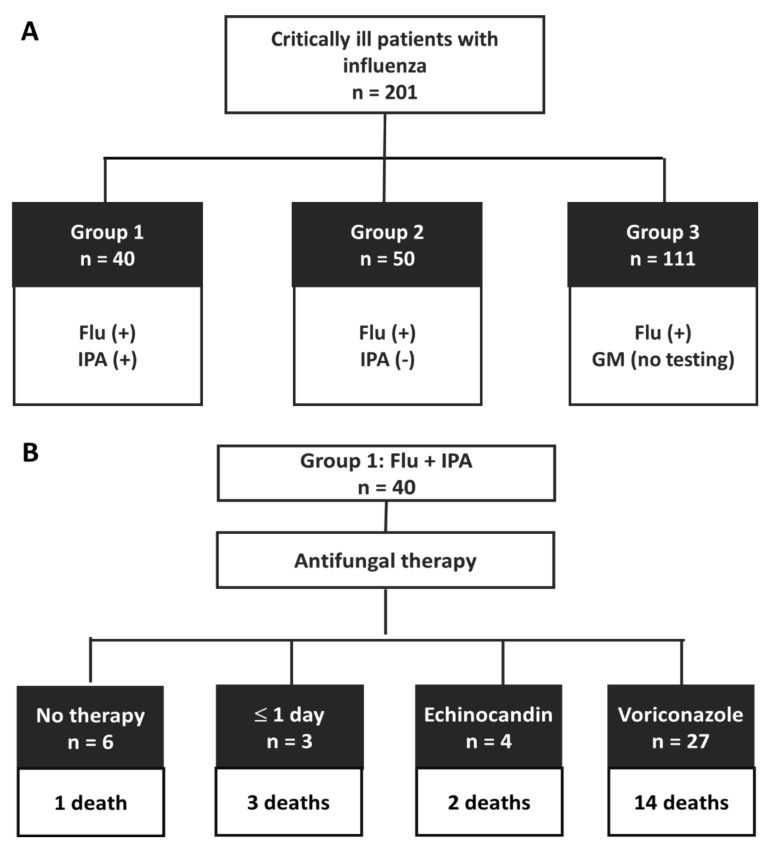
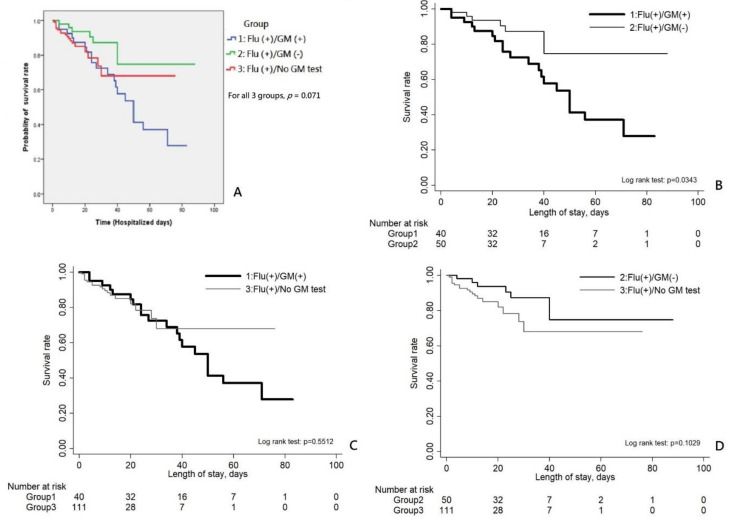
Previous studies have revealed higher mortality rates in patients with severe influenza who are coinfected with invasive pulmonary aspergillosis (IPA) than in those without IPA coinfection; nonetheless, the clinical impact of IPA on economic burden and risk factors for mortality in critically ill influenza patients remains undefined. The study was retrospectively conducted in three institutes. From 2016 through 2018, all adult patients with severe influenza admitted to an intensive care unit (ICU) were identified. All patients were classified as group 1, patients with concomitant severe influenza and IPA; group 2, severe influenza patients without IPA; and group 3, severe influenza patients without testing for IPA. Overall, there were 201 patients enrolled, including group 1 (n = 40), group 2 (n = 50), and group 3 (n = 111). Group 1 patients had a significantly higher mortality rate (20/40, 50%) than that of group 2 (6/50, 12%) and group 3 (18/11, 16.2%), p < 0.001. The risk factors for IPA occurrence were solid cancer and prolonged corticosteroid use in ICU of >5 days. Group 1 patients had significantly longer hospital stay and higher medical expenditure than the other two groups. The risk factors for mortality in group 1 patients included patients' Charlson comorbidity index, presenting APACHE II score, and complication of severe acute respiratory distress syndrome. Overall, IPA has a significant adverse impact on the outcome and economic burden of severe influenza patients, who should be promptly managed based on risk host factors for IPA occurrence and mortality risk factors for coinfection with both diseases.
Keywords: aspergillosis; influenza; intensive care unit; mortality; outcome.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
LinkOut - more resources
Full Text Sources
