

Fungal Endophthalmitis: A Comprehensive Review
- PMID: 34829283
- PMCID: PMC8623405
- DOI: 10.3390/jof7110996
Fungal Endophthalmitis: A Comprehensive Review
Abstract
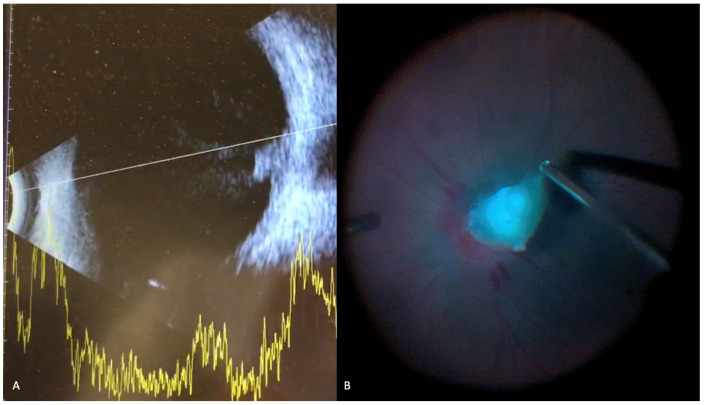
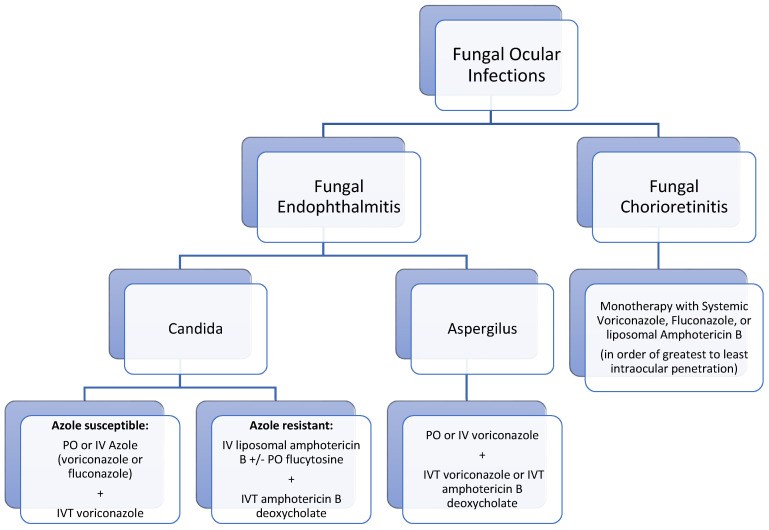
Endophthalmitis is a serious ophthalmologic condition involving purulent inflammation of the intraocular spaces. The underlying etiology of infectious endophthalmitis is typically bacterial or fungal. The mechanism of entry into the eye is either exogenous, involving seeding of an infectious source from outside the eye (e.g., trauma or surgical complications), or endogenous, involving transit of an infectious source to the eye via the bloodstream. The most common organism for fungal endophthalmitis is Candida albicans. The most common clinical manifestation of fungal endophthalmitis is vision loss, but other signs of inflammation and infection are frequently present. Fungal endophthalmitis is a clinical diagnosis, which can be supported by vitreous, aqueous, or blood cultures. Treatment involves systemic and intravitreal antifungal medications as well as possible pars plana vitrectomy. In this review, we examine these essential elements of understanding fungal endophthalmitis as a clinically relevant entity, which threatens patients' vision.
Keywords: Aspergillus; Candida; antifungals; endogenous endophthalmitis; exogenous endophthalmitis; fungal endophthalmitis; pars plana vitrectomy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
