

Idiopathic Megacolon-Short Review
- PMID: 34829459
- PMCID: PMC8622596
- DOI: 10.3390/diagnostics11112112
Idiopathic Megacolon-Short Review
Abstract
Introduction: Idiopathic megacolon (IM) is a rare condition with a more or less known etiology, which involves management challenges, especially therapeutic, and both gastroenterology and surgery services. With insufficiently drawn out protocols, but with occasionally formidable complications, the condition management can be difficult for any general surgery team, either as a failure of drug therapy (in the context of a known case, initially managed by a gastroenterologist) or as a surgical emergency (in which the diagnostic surprise leads additional difficulties to the tactical decision), when the speed imposed by the severity of the case can lead to inadequate strategies, with possibly critical consequences.
Method: With such a motivation, and having available experience limited by the small number of cases (described by all medical teams concerned with this pathology), the revision of the literature with the update of management landmarks from the surgical perspective of the pathology appears as justified by this article.
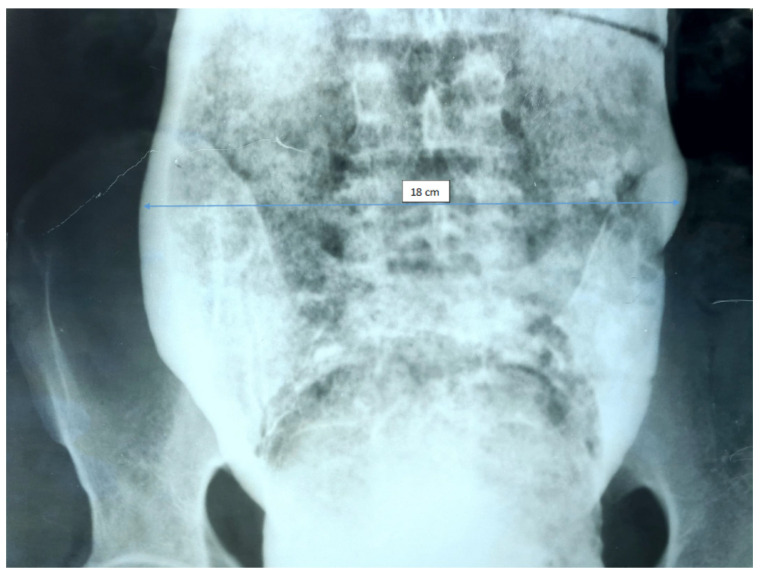
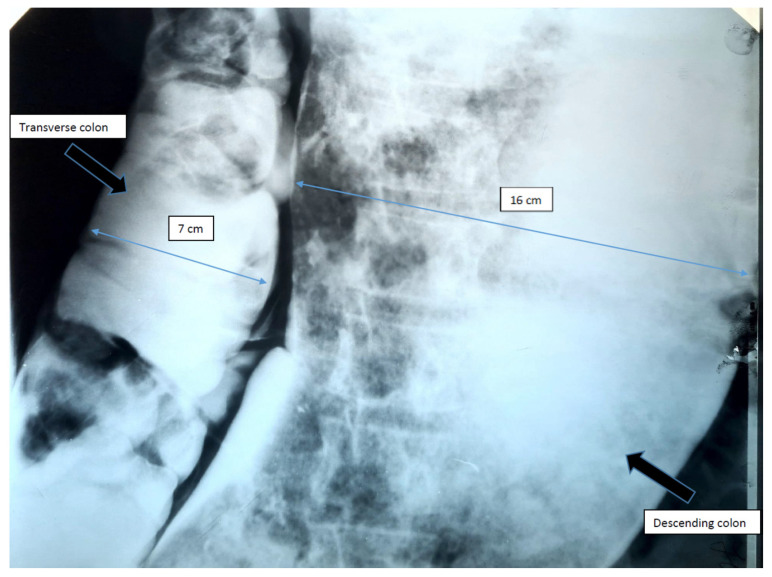
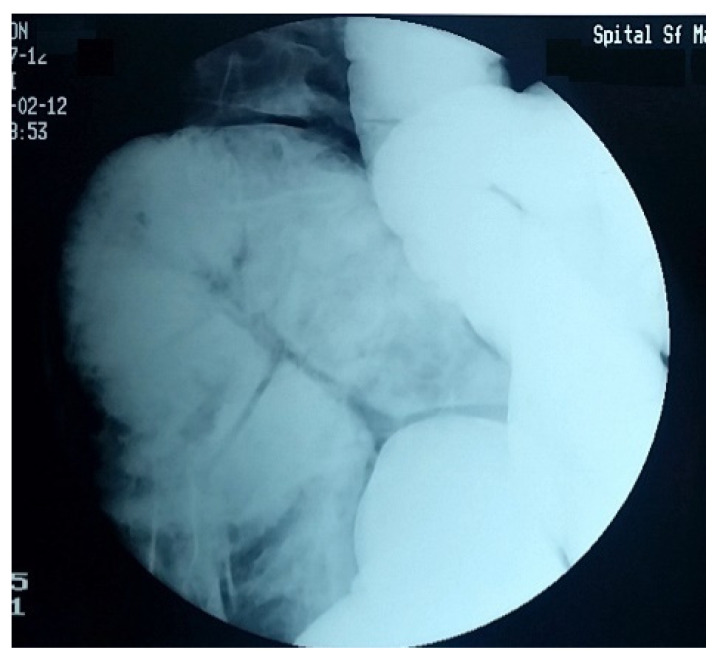
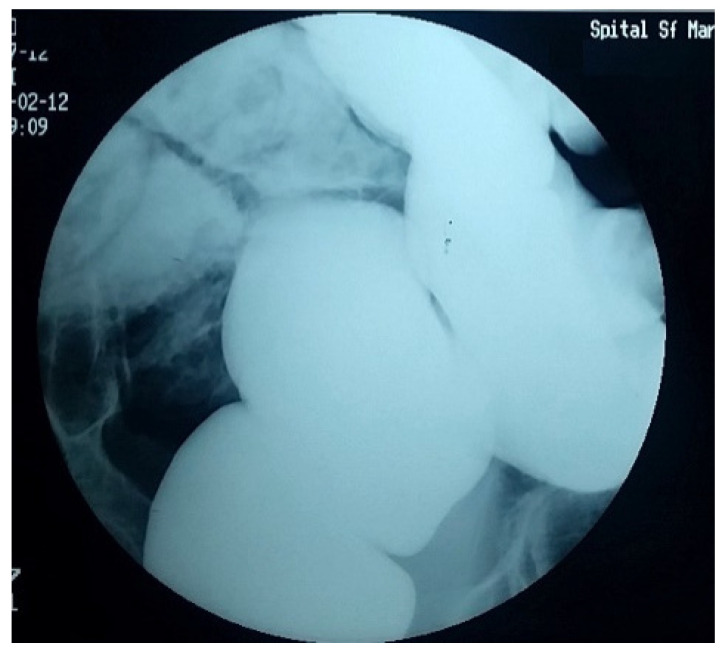
Results: If the diagnosis of megacolon is made relatively easily by imaging the colorectal dilation (which is associated with initial and/or consecutive clinical aspects), the establishing of the diagnosis of idiopathic megacolon is based in practice almost exclusively on a principle of exclusion, and after evaluating the absence of some known causes that can lead to the occurrence of these anatomic and clinical changes, mimetically, clinically, and paraclinically, with IM (intramural aganglionosis, distal obstructions, intoxications, etc.). If the etiopathogenic theories, based on an increase in the performance of the arsenal of investigations of the disease, have registered a continuous improvement and an increase of objectivity, unfortunately, the curative surgical treatment options still revolve around the same resection techniques. Moreover, the possibility of developing a form of etiopathogenic treatment seems as remote as ever.
Keywords: etiopathogenic theories of idiopathic megacolon; idiopathic megacolon; surgical treatment.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
Publication types
LinkOut - more resources
Full Text Sources
