

Immunotherapy in Breast Cancer: When, How, and What Challenges?
- PMID: 34829916
- PMCID: PMC8616011
- DOI: 10.3390/biomedicines9111687
Immunotherapy in Breast Cancer: When, How, and What Challenges?
Abstract
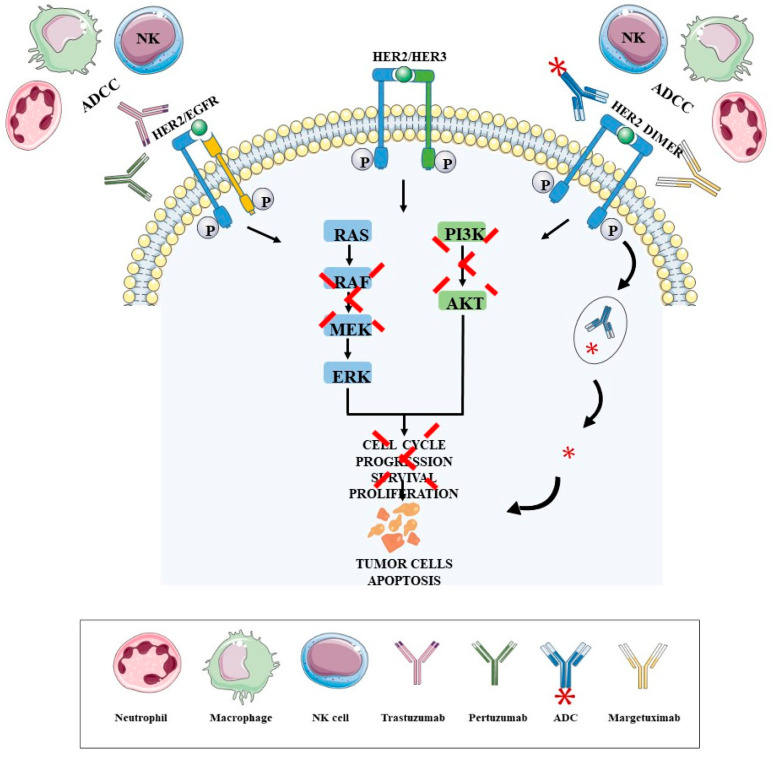
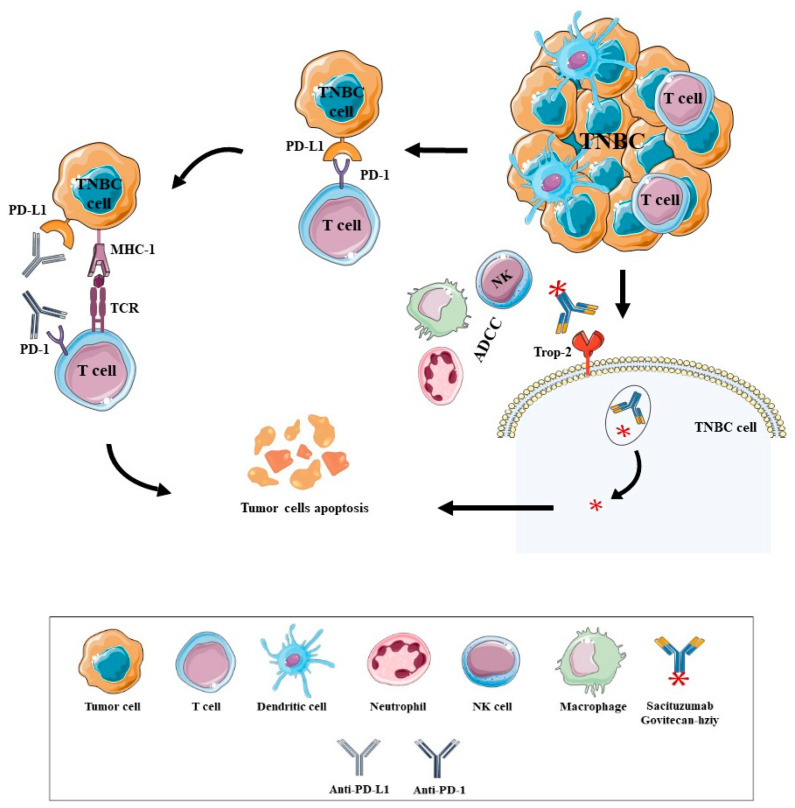
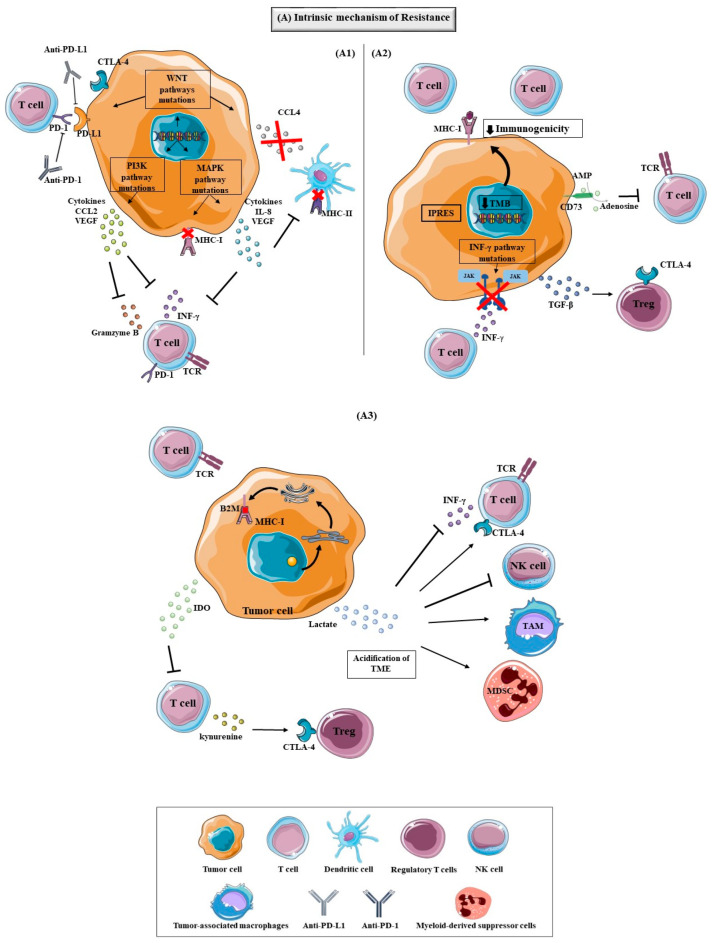
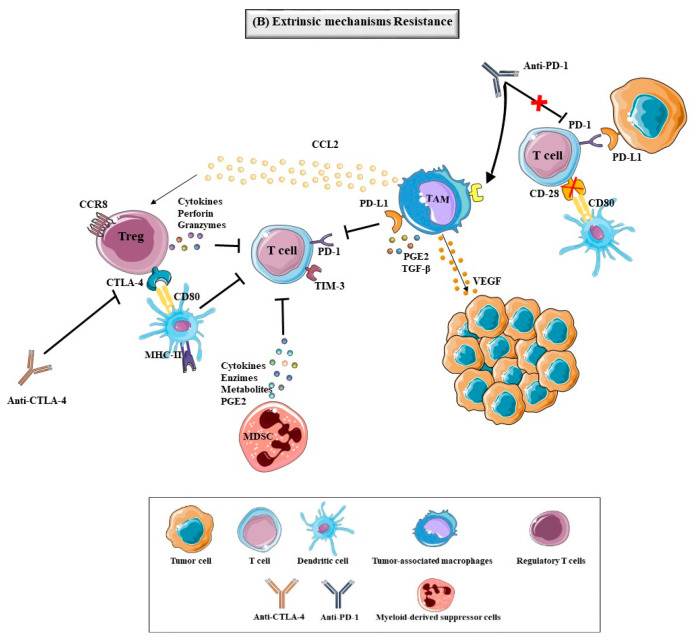
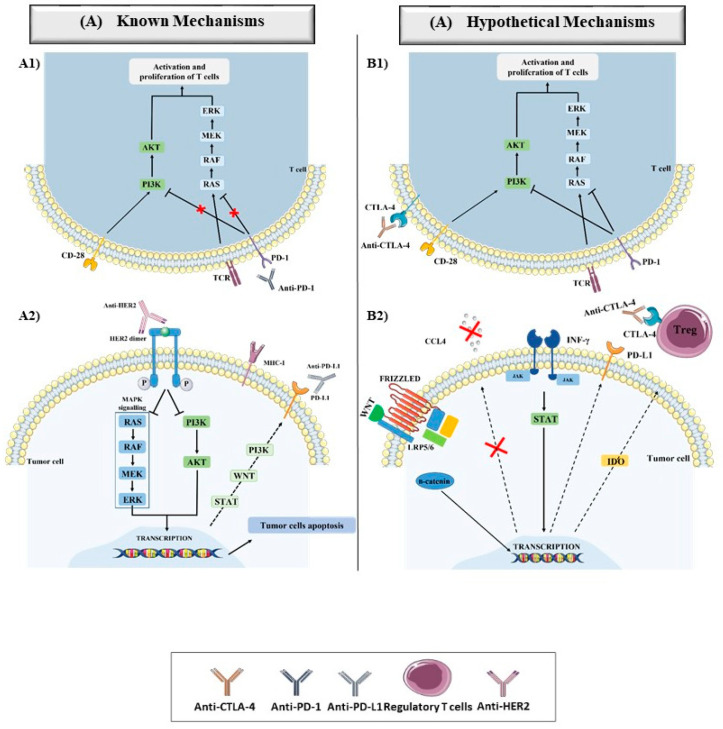
Breast Cancer (BC) is the second most frequent cause of cancer death among women worldwide and, although there have been significant advances in BC therapies, a significant percentage of patients develop metastasis and disease recurrence. Since BC was demonstrated to be an immunogenic tumor, immunotherapy has broken through as a significant therapy strategy against BC. Over the years, immunotherapy has improved the survival rate of HER2+ BC patients due to the approval of some monoclonal antibodies (mAbs) such as Trastuzumab, Pertuzumab and, recently, Margetuximab, along with the antibody-drug conjugates (ADC) Trastuzumab-Emtansine (T-DM1) and Trastuzumab Deruxtecan. Immune checkpoint inhibitors (ICI) showed promising efficacy in triple-negative breast cancer (TNBC) treatment, namely Atezolizumab and Pembrolizumab. Despite the success of immunotherapy, some patients do not respond to immunotherapy or those who respond to the treatment relapse or progress. The main causes of these adverse events are the complex, intrinsic or extrinsic resistance mechanisms. In this review, we address the different immunotherapy approaches approved for BC and some of the mechanisms responsible for resistance to immunotherapy.
Keywords: breast cancer; immunotherapy; therapeutic resistance.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Feng Y., Spezia M., Huang S., Yuan C., Zeng Z., Zhang L., Ji X., Liu W., Huang B., Luo W., et al. Breast cancer development and progression: Risk factors, cancer stem cells, signaling pathways, genomics, and molecular pathogenesis. Genes Dis. 2018;5:77–106. doi: 10.1016/j.gendis.2018.05.001. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
