

Emerging Approaches for Solid Tumor Treatment Using CAR-T Cell Therapy
- PMID: 34830003
- PMCID: PMC8621681
- DOI: 10.3390/ijms222212126
Emerging Approaches for Solid Tumor Treatment Using CAR-T Cell Therapy
Abstract
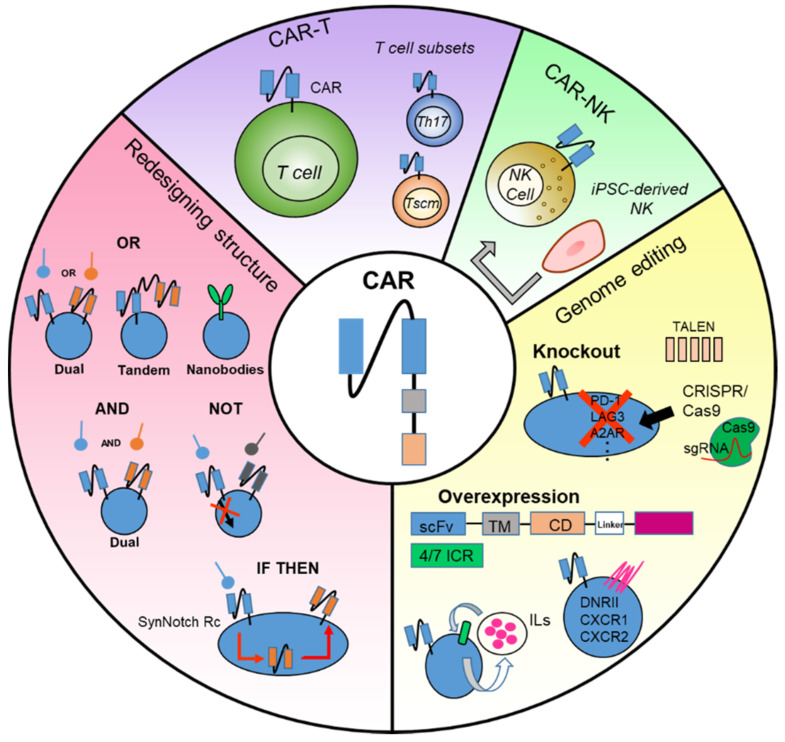
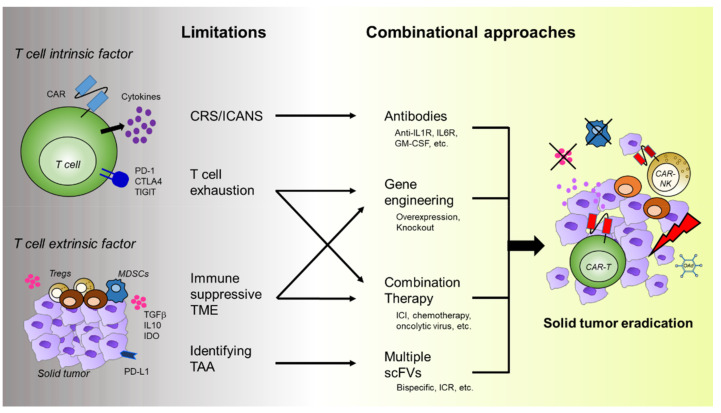
Cancer immunotherapy is becoming more important in the clinical setting, especially for cancers resistant to conventional chemotherapy, including targeted therapy. Chimeric antigen receptor (CAR)-T cell therapy, which uses patient's autologous T cells, combined with engineered T cell receptors, has shown remarkable results, with five US Food and Drug Administration (FDA) approvals to date. CAR-T cells have been very effective in hematologic malignancies, such as diffuse large B cell lymphoma (DLBCL), B cell acute lymphoblastic leukemia (B-ALL), and multiple myeloma (MM); however, its effectiveness in treating solid tumors has not been evaluated clearly. Therefore, many studies and clinical investigations are emerging to improve the CAR-T cell efficacy in solid tumors. The novel therapeutic approaches include modifying CARs in multiple ways or developing a combination therapy with immune checkpoint inhibitors and chemotherapies. In this review, we focus on the challenges and recent advancements in CAR-T cell therapy for solid tumors.
Keywords: CAR-T cell; challenge; combination therapy; solid tumor.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- 2016R1C1B3009116/National Research Foundation of Korea
- 2021R1C1C1011899/National Research Foundation of Korea
- 2020R1A2C2012467/National Research Foundation of Korea
- KGS1352113/Korea Research Institute of Bioscience and Biotechnology
- KGM5362111/Korea Research Institute of Bioscience and Biotechnology
LinkOut - more resources
Full Text Sources
Other Literature Sources
