

Kinase-Inhibitors in Iodine-Refractory Differentiated Thyroid Cancer-Focus on Occurrence, Mechanisms, and Management of Treatment-Related Hypertension
- PMID: 34830100
- PMCID: PMC8623313
- DOI: 10.3390/ijms222212217
Kinase-Inhibitors in Iodine-Refractory Differentiated Thyroid Cancer-Focus on Occurrence, Mechanisms, and Management of Treatment-Related Hypertension
Abstract
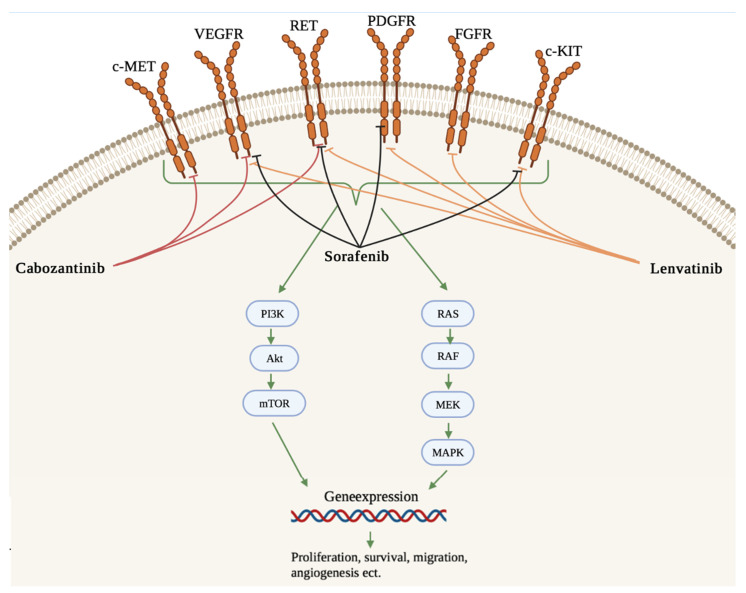
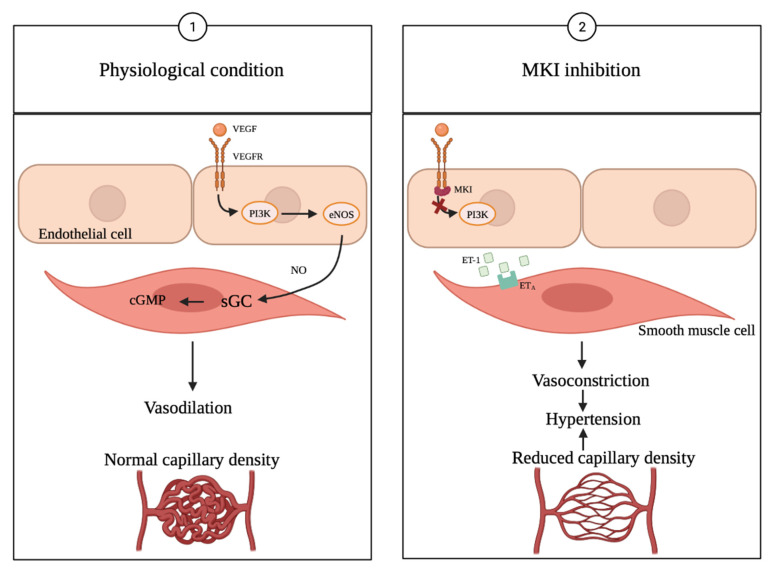
Differentiated thyroid cancer (DTC) usually has a good prognosis when treated conventionally with thyroidectomy, radioactive iodine (RAI) and thyroid-stimulating hormone suppression, but some tumors develop a resistance to RAI therapy, requiring alternative treatments. Sorafenib, lenvatinib and cabozantinib are multikinase inhibitors (MKIs) approved for the treatment of RAI-refractory DTC. The drugs have been shown to improve progression-free survival (PFS) and overall survival (OS) via the inhibition of different receptor tyrosine kinases (RTKs) that are involved in tumorigenesis and angiogenesis. Both sorafenib and lenvatinib have been approved irrespective of the line of therapy for the treatment of RAI-refractory DTC, whereas cabozantinib has only been approved as a second-line treatment. Adverse effects (AEs) such as hypertension are often seen with MKI treatment, but are generally well manageable. In this review, current clinical studies will be discussed, and the toxicity and safety of sorafenib, lenvatinib and cabozantinib treatment will be evaluated, with a focus on AE hypertension and its treatment options. In short, treatment-emergent hypertension (TE-HTN) occurs with all three drugs, but is usually well manageable and leads only to a few dose modifications or even discontinuations. This is emphasized by the fact that lenvatinib is widely considered the first-line drug of choice, despite its higher rate of TE-HTN.
Keywords: adverse effects; cabozantinib; hypertension; lenvatinib; multikinase inhibitors; sorafenib; thyroid cancer.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
