

Injuries during Laparoscopic Cholecystectomy: A Scoping Review of the Claims and Civil Action Judgements
- PMID: 34830520
- PMCID: PMC8622805
- DOI: 10.3390/jcm10225238
Injuries during Laparoscopic Cholecystectomy: A Scoping Review of the Claims and Civil Action Judgements
Abstract
Background: To define what type of injuries are more frequently related to medicolegal claims and civil action judgments.
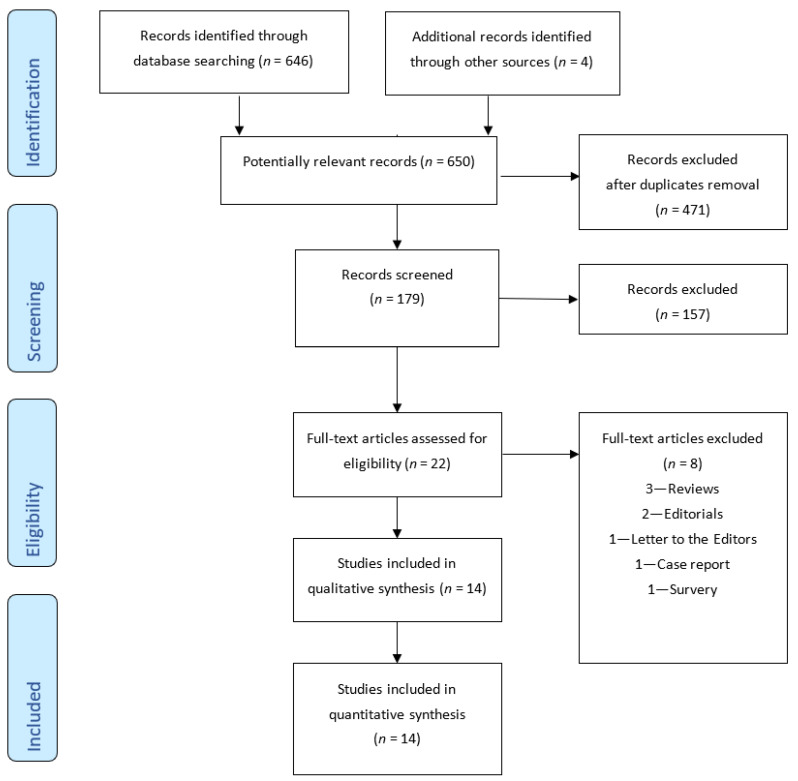
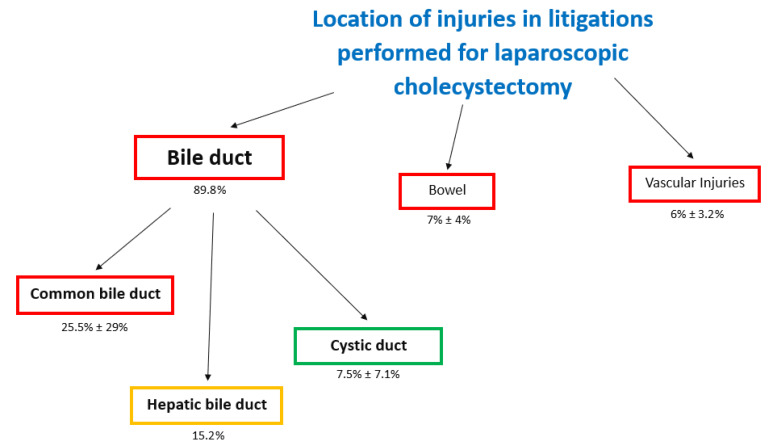
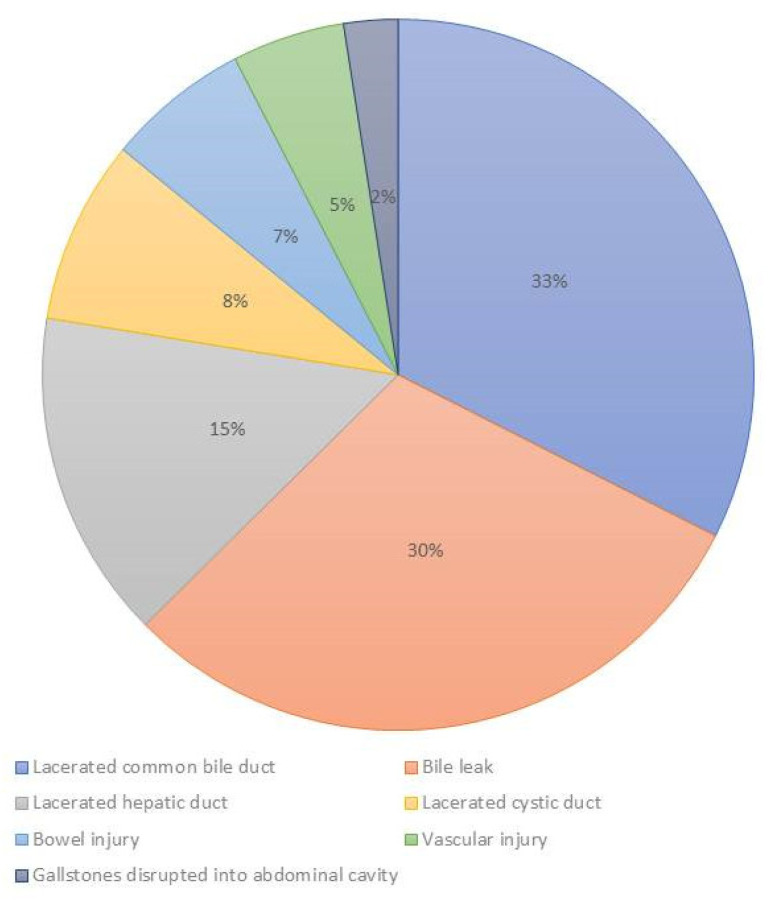
Methods: We performed a scoping review on 14 studies and 2406 patients, analyzing medicolegal claims related to laparoscopic cholecystectomy injuries. We have focalized on three phases associated with claims: phase of care, location of injuries, type of injuries.
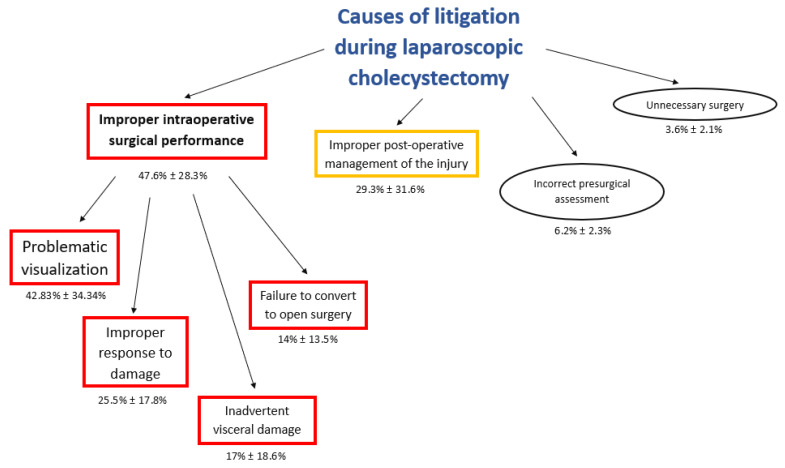
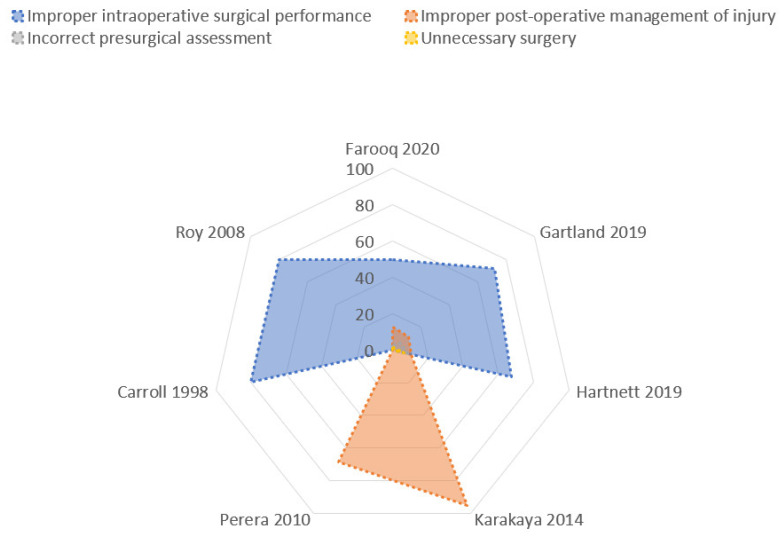
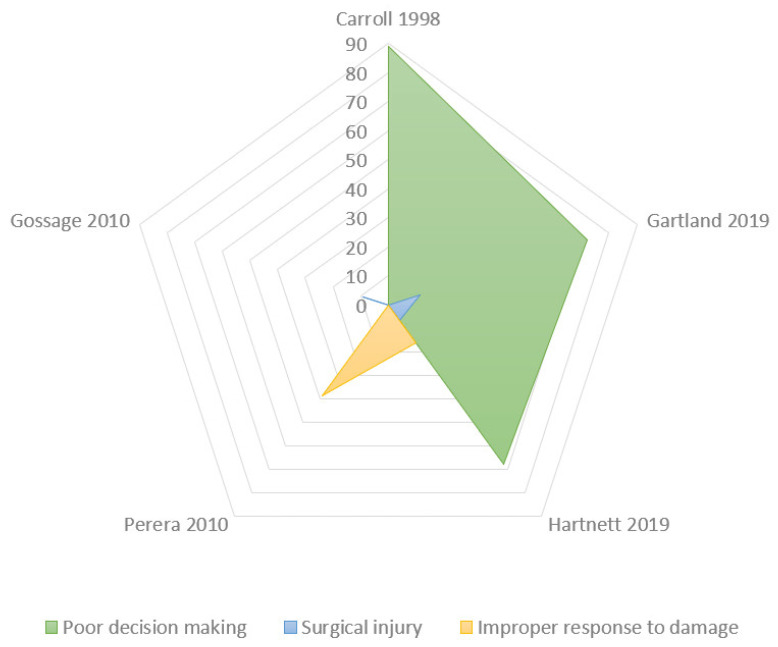
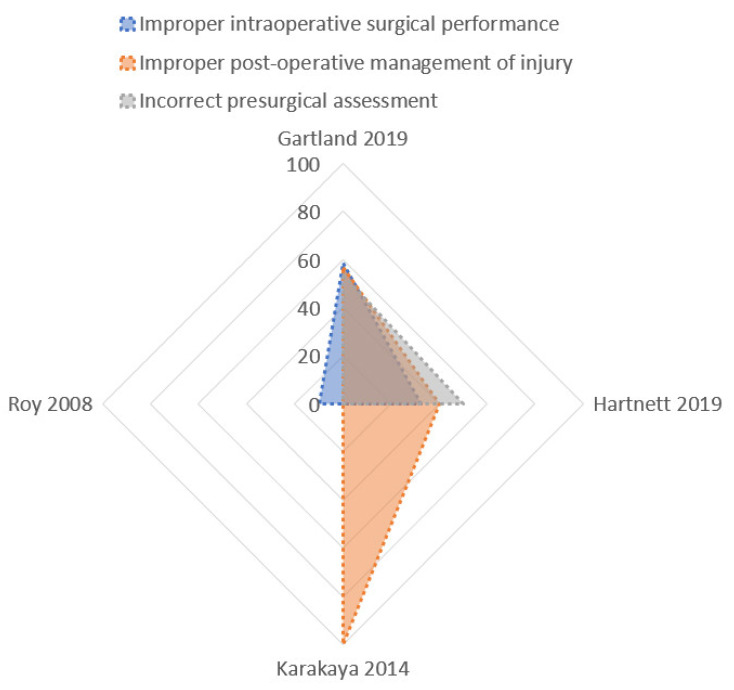
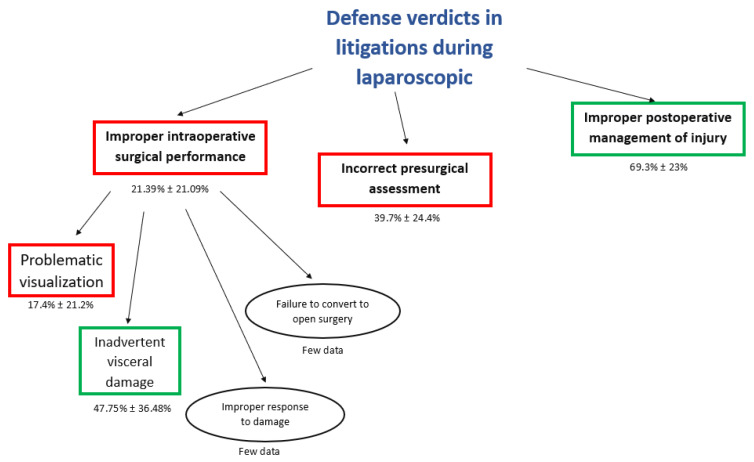
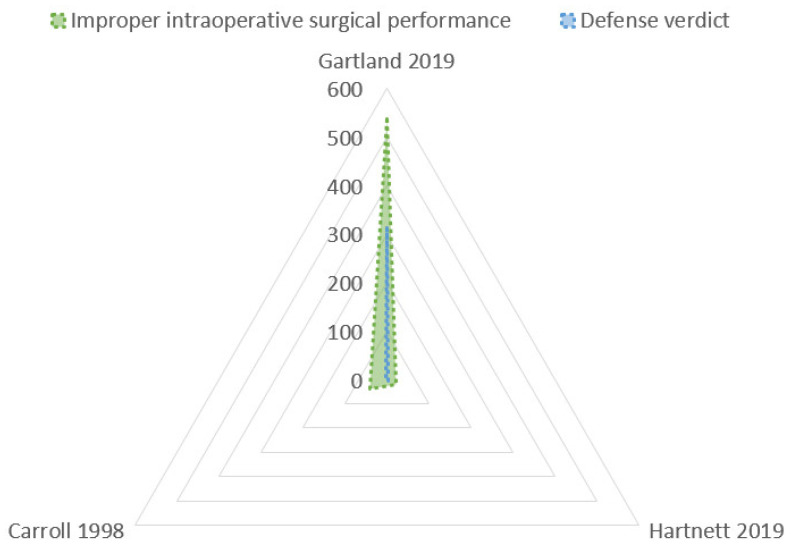
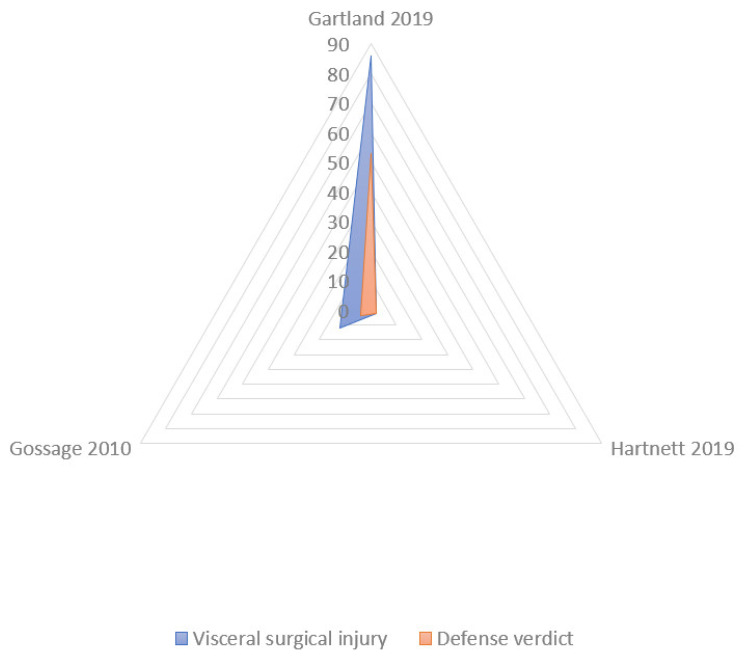
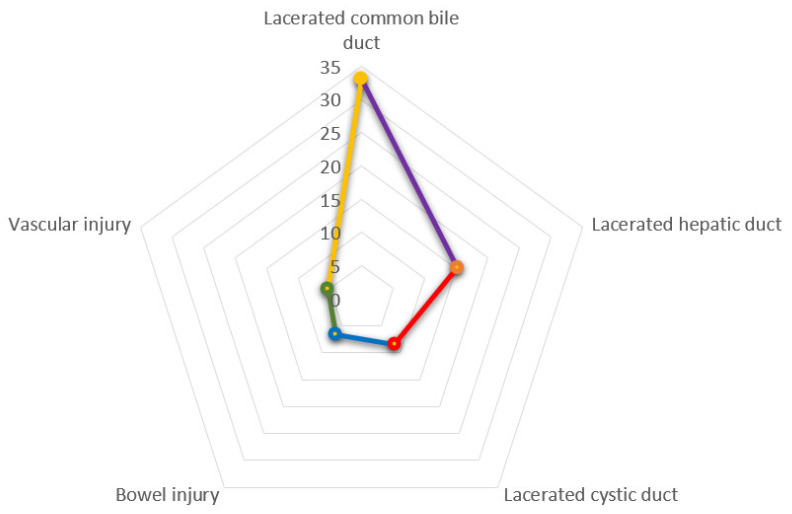
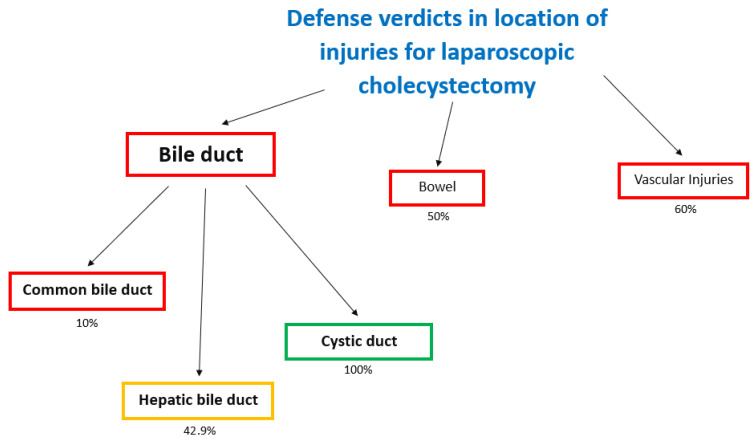
Results: The most common phase of care associated with litigation was the improper intraoperative surgical performance (47.6% ± 28.3%), related to a "poor" visualization, and the improper post-operative management (29.3% ± 31.6%). The highest rate of defense verdicts was reported for the improper post-operative management of the injury (69.3% ± 23%). A lower rate was reported in the incorrect presurgical assessment (39.7% ± 24.4%) and in the improper intraoperative surgical performance (21.39% ± 21.09%). A defense verdict was more common in cystic duct injuries (100%), lower in hepatic bile duct (42.9%) and common bile duct (10%) injuries.
Conclusions: During laparoscopic cholecystectomy, the most common cause of claims, associated with lower rate of defense verdict, was the improper intraoperative surgical performance. The decision to take legal action was determined often for poor communication after the original incident.
Keywords: biliary injury; laparoscopic cholecystectomy; legal practice; litigation; postoperative complications.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
