

Three-Device (3D) Technique for Liver Parenchyma Dissection in Robotic Liver Surgery
- PMID: 34830547
- PMCID: PMC8653962
- DOI: 10.3390/jcm10225265
Three-Device (3D) Technique for Liver Parenchyma Dissection in Robotic Liver Surgery
Abstract
Background: The implementation of robotics in liver surgery offers several advantages compared to conventional open and laparoscopic techniques. One major advantage is the enhanced degree of freedom at the tip of the robotic tools compared to laparoscopic instruments. This enables excellent vessel control during inflow and outflow dissection of the liver. Parenchymal transection remains the most challenging part during robotic liver resection because currently available robotic instruments for parenchymal transection have several limitations and there is no standardized technique as of yet. We established a new strategy and share our experience.
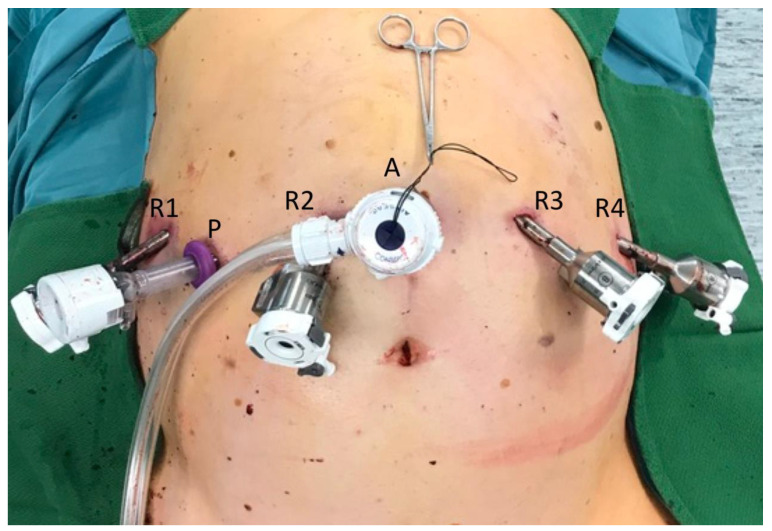
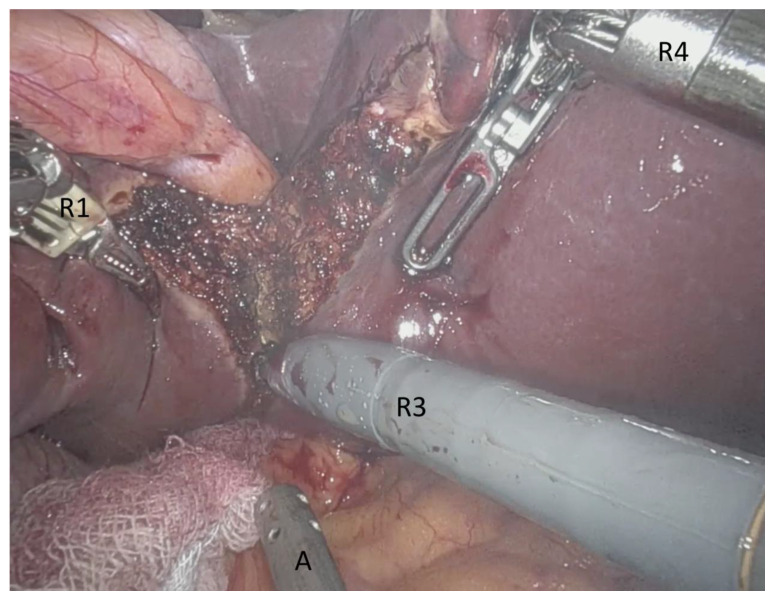
Methods: We present a novel technique for the transection of liver parenchyma during robotic surgery, using three devices (3D) simultaneously: monopolar scissors and bipolar Maryland forceps of the robot and laparoscopic-guided waterjet. We collected the perioperative data of twenty-eight patients who underwent this procedure for minor and major liver resections between February 2019 and December 2020 from the Magdeburg Registry of minimally invasive liver surgery (MD-MILS).
Results: Twenty-eight patients underwent robotic-assisted 3D parenchyma dissection within the investigation period. Twelve cases of major and sixteen cases of minor hepatectomy for malignant and non-malignant cases were performed. Operative time for major liver resections (≥ 3 liver segments) was 381.7 (SD 80.6) min vs. 252.0 (70.4) min for minor resections (p < 0.01). Intraoperative measured blood loss was 495.8 (SD 508.8) ml for major and 256.3 (170.2) ml for minor liver resections (p = 0.090). The mean postoperative stay was 13.3 (SD 11.1) days for all cases. Liver surgery-related morbidity was 10.7%, no mortalities occurred. We achieved an R0 resection in all malignant cases.
Conclusions: The 3D technique for parenchyma dissection in robotic liver surgery is a safe and feasible procedure. This novel method offers an advanced locally controlled preparation of intrahepatic vessels and bile ducts. The combination of precise extrahepatic vessel handling with the 3D technique of parenchyma dissection is a fundamental step forward to the standardization of robotic liver surgery for teaching purposing and the wider adoption of robotic hepatectomy into routine patient care.
Keywords: hepatectomy; hepatocellular carcinoma; liver metastasis; liver surgery; robotic surgery.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Gigot J.-F., Glineur D., Azagra J.S., Goergen M., Ceuterick M., Morino M., Etienne J., Marescaux J., Mutter D., van Krunckelsven L., et al. Laparoscopic liver resection for malignant liver tumors: Preliminary results of a multicenter European study. Ann. Surg. 2002;236:90–97. doi: 10.1097/00000658-200207000-00014. - DOI - PMC - PubMed
-
- Wakabayashi G., Cherqui D., Geller D.A., Buell J.F., Kaneko H., Han H.S., Asbun H., O’Rourke N., Tanabe M., Koffron A.J., et al. Recommendations for laparoscopic liver resection: A report from the second international consensus conference held in Morioka. Ann. Surg. 2015;261:619–629. - PubMed
LinkOut - more resources
Full Text Sources
