

Other (Non-CNS/Testicular) Extramedullary Localizations of Childhood Relapsed Acute Lymphoblastic Leukemia and Lymphoblastic Lymphoma-A Report from the ALL-REZ Study Group
- PMID: 34830574
- PMCID: PMC8621955
- DOI: 10.3390/jcm10225292
Other (Non-CNS/Testicular) Extramedullary Localizations of Childhood Relapsed Acute Lymphoblastic Leukemia and Lymphoblastic Lymphoma-A Report from the ALL-REZ Study Group
Abstract
Children with other extramedullary relapse of acute lymphoblastic leukemia are currently poorly characterized. We aim to assess the prevalence and the clinical, therapeutic and prognostic features of extramedullary localizations other than central nervous system or testis in children with relapse of acute lymphoblastic leukemia (ALL) and lymphoblastic lymphoma (LBL) treated on a relapsed ALL protocol.
Patients and methods: Patients with relapse of ALL and LBL, treated according to the multicentric ALL-REZ BFM trials between 1983 and 2015, were analyzed for other extramedullary relapse (OEMR) of the disease regarding clinical features, treatment and outcome. Local treatment/irradiation has been recommended on an individual basis and performed only in a minority of patients.
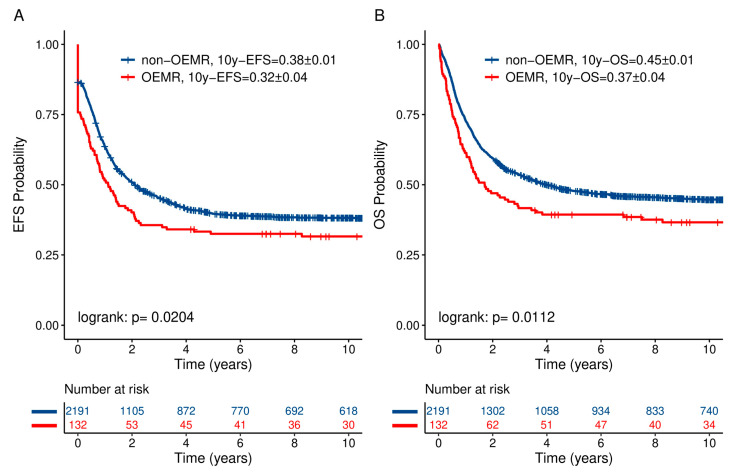
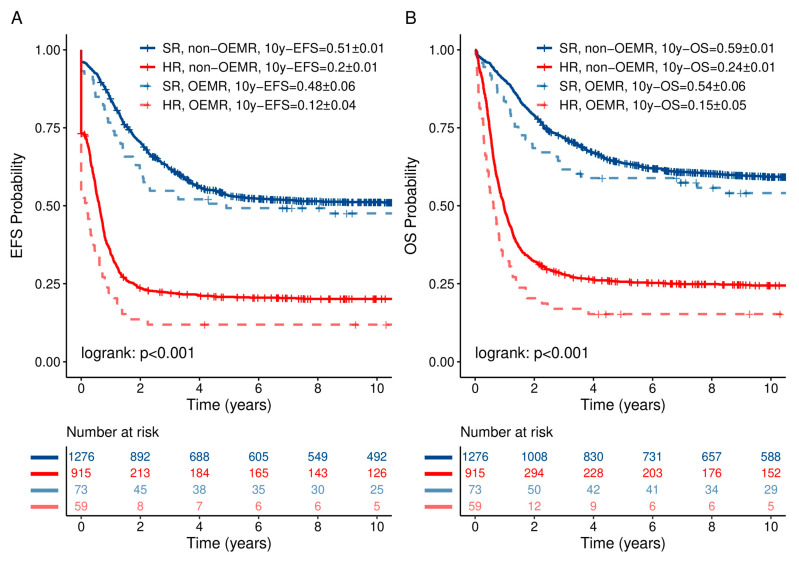
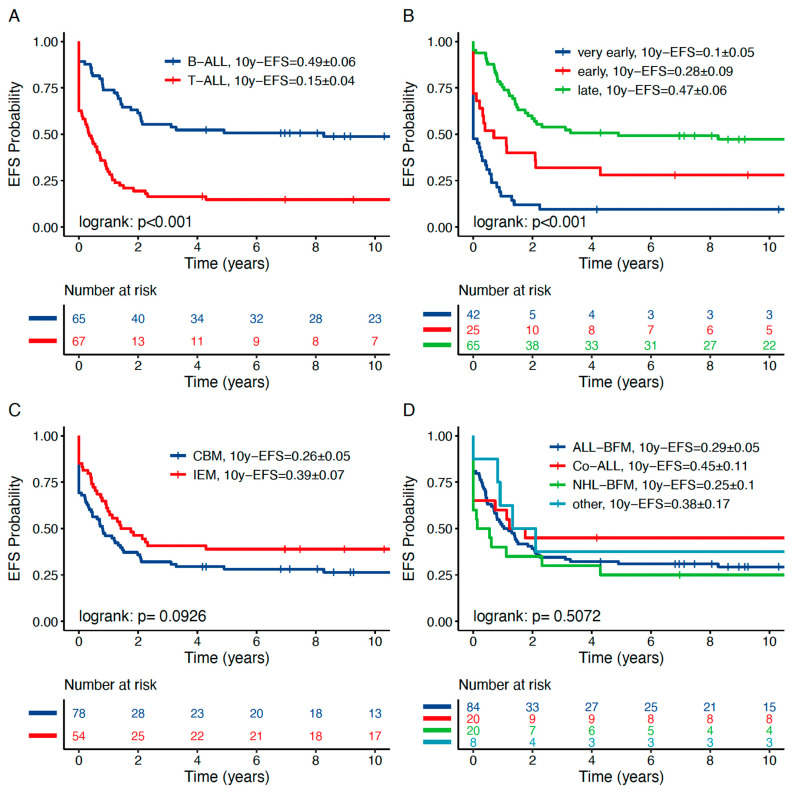
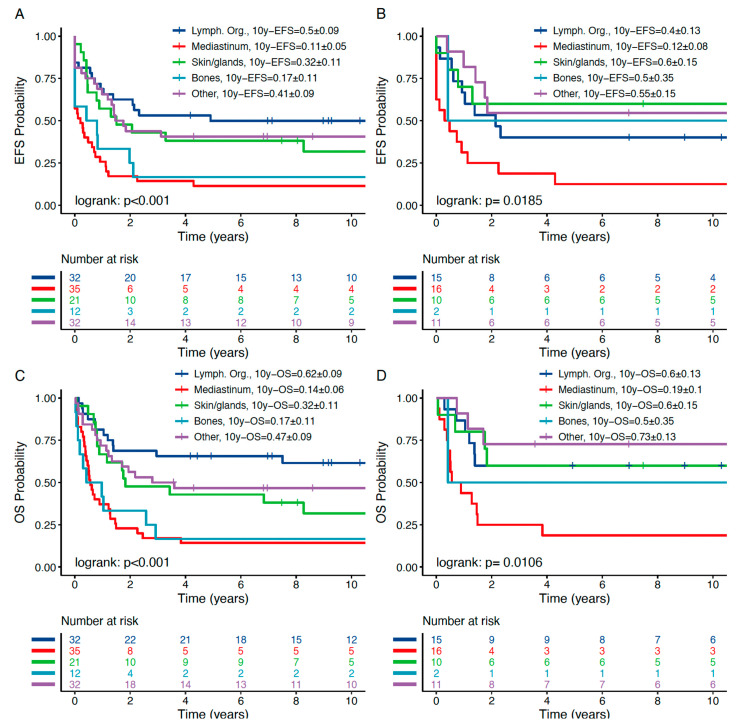
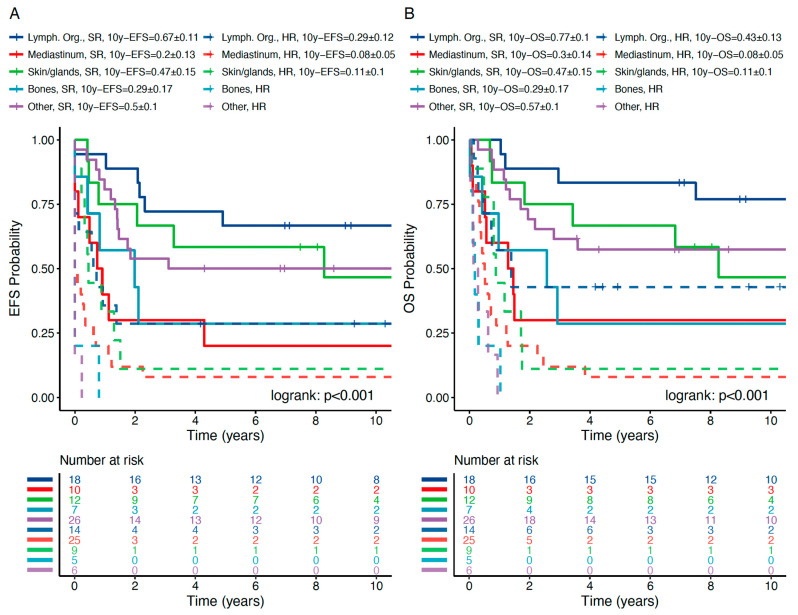
Results: A total of 132 out of 2323 (5.6%) patients with ALL relapse presented with an OEMR (combined bone marrow relapse n = 78; isolated extramedullary relapse n = 54). Compared to the non-OEMR group, patients with OEMR had a higher rate of T-immunophenotype (p < 0.001), a higher rate of LBL (p < 0.001) and a significantly different distribution of time to relapse, i.e., more very early and late relapses compared to the non-OEMR group (p = 0.01). Ten-year probabilities of event-free survival (pEFS) and overall survival (pOS) in non-OEMR vs. OEMR were 0.38 ± 0.01 and 0.32 ± 0.04 (p = 0.0204) vs. 0.45 ± 0.01 and 0.37 ± 0.04 (p = 0.0112), respectively. OEMRs have been classified into five subgroups according to the main affected compartment: lymphatic organs (n = 32, 10y-pEFS 0.50 ± 0.09), mediastinum (n = 35, 10y-pEFS 0.11 ± 0.05), bone (n = 12, 0.17 ± 0.11), skin and glands (n = 21, 0.32 ± 0.11) and other localizations (n = 32, 0.41 ± 0.09). Patients with OEMR and T-lineage ALL/LBL showed a significantly worse 10y-pEFS (0.15 ± 0.04) than those with B-Precursor-ALL (0.49 ± 0.06, p < 0.001). Stratified into standard risk (SR) and high risk (HR) groups, pEFS and pOS of OEMR subgroups were in the expected range whereas the mediastinal subgroup had a significantly worse outcome. Subsequent relapses involved more frequently the bone marrow (58.4%) than isolated extramedullary compartments (41.7%). In multivariate Cox regression, OEMR confers an independent prognostic factor for inferior pEFS and pOS.
Conclusion: OEMR is adversely related to prognosis. However, the established risk classification can be applied for all subgroups except mediastinal relapses requiring treatment intensification. Generally, isolated OEMR of T-cell-origin needs an intensified treatment including allogeneic stem cell transplantation (HSCT) as a curative approach independent from time to relapse. Local therapy such as surgery and irradiation may be of benefit in selected cases. The indication needs to be clarified in further investigations.
Keywords: lymphoblastic leukemia; other extramedullary relapse; pediatric.
Conflict of interest statement
The authors have no competing interest. The authors declare no conflict of interest.
Figures
References
-
- Wofford M.M., Smith S.D., Shuster J.J., Johnson W., Buchanan G.R., Wharam M.D., Ritchey A.K., Rosen D., Haggard M.E., Golembe B.L., et al. Treatment of occult or late overt testicular relapse in children with acute lymphoblastic leukemia: A Pediatric Oncology Group study. J. Clin. Oncol. 1992;10:624–630. doi: 10.1200/JCO.1992.10.4.624. - DOI - PubMed
-
- Murray J.C., Gmoser D.J., Barnes D.A., Oshman D., Hawkins H.K., Gresik M.V., Dreyer Z.E. Isolated bone relapse during hematologic remission in childhood acute lymphoblastic leukemia: Report of a metatarsal relapse and review of the literature. Med. Pediatr. Oncol. 1994;23:153–157. doi: 10.1002/mpo.2950230217. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
