

Facilitators and Strategies for Breaking the News of an Intrauterine Death-A Mixed Methods Study among Obstetricians
- PMID: 34830629
- PMCID: PMC8625483
- DOI: 10.3390/jcm10225347
Facilitators and Strategies for Breaking the News of an Intrauterine Death-A Mixed Methods Study among Obstetricians
Abstract
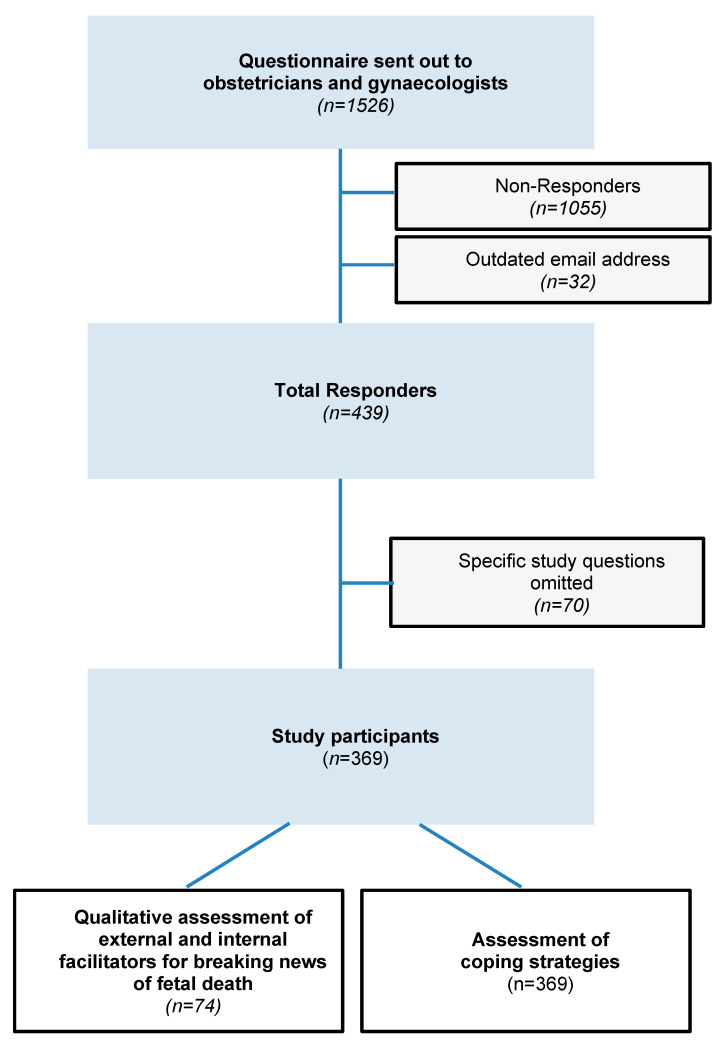
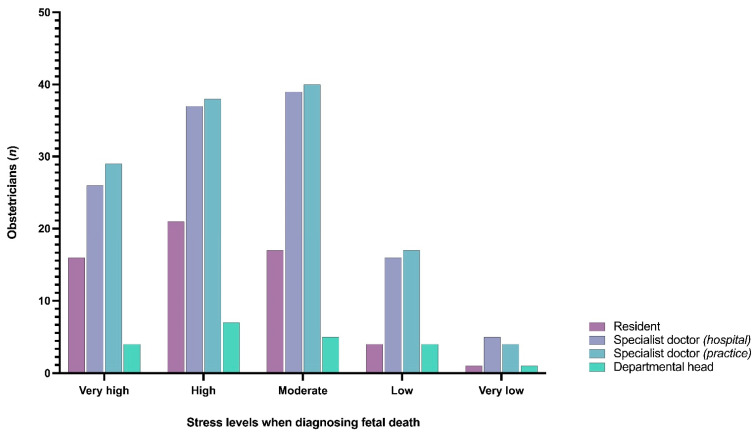
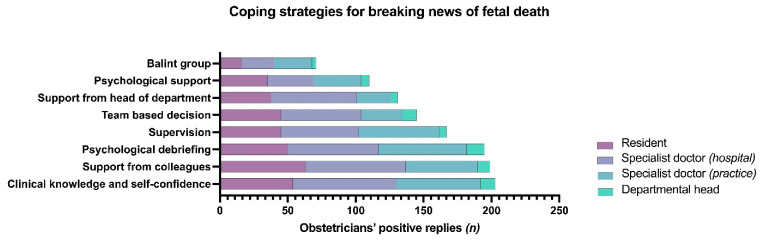
(1) Background: The death of a baby in utero is a very sad event for both the affected parents and the caring doctors. By this study, we aimed to assess the tools, which may help obstetricians to overcome this challenge in their profession. (2) Methods: We conducted a cross-sectional online survey in 1526 obstetricians registered with the Austrian Society of Obstetrics and Gynecology between September and October 2020. (3) Results: With a response rate of 24.2% (n = 439), our study shows that diagnosing fetal death was associated with a moderate to high degree of stress, regardless of position (p = 0.949), age (p = 0.110), gender (p = 0.155), and experience (p = 0.150) of physicians. Coping strategies for delivering the news of intrauterine death to affected parents were relying on clinical knowledge and high levels of self-confidence (55.0%; 203/369), support from colleagues (53.9%; 199/369), and debriefing (52.8%; 195/369). In general, facilitators for breaking bad news were more commonly cultivated by female obstetricians [OR 1.267 (95% CI 1.149-1.396); p < 0.001], residents [χ2(3;369) = 9.937; p = 0.019], and obstetricians of younger age [41 (34-50) years vs. 45 (36-55) years; p = 0.018]. External facilitators were most frequently mentioned, including professional support, training, professional guidance, time, parents' leaflets, follow-up consultations, a supporting consultation atmosphere, and preparation before delivering the bad news. Internal facilitators included knowledge, empathy, seeking silence, reflection, privacy, and relief of guilt. (4) Conclusions: Communicating the diagnosis of fetal death evokes moderate to high levels of stress among obstetricians. Resources from both the professional and private environment are required to deal with this professional challenge on a personal level.
Keywords: breaking bad news; coping strategies; fetal death; intrauterine death; resilience; stillbirth; stress.
Conflict of interest statement
The authors declare no conflict of interest. No funding was received for conduction of this study.
Figures


Similar articles
-
Personality traits and stress coping among obstetricians diagnosing and communicating fetal death: A cross-sectional study.Int J Gynaecol Obstet. 2022 Aug;158(2):453-461. doi: 10.1002/ijgo.14048. Epub 2021 Dec 11. Int J Gynaecol Obstet. 2022. PMID: 34837223 Free PMC article.
-
Addressing obstetricians' awareness of compassion, communication, and self-care when caring for families experiencing stillbirth: Evaluation of a novel educational workshop using applied drama techniques.PLoS One. 2022 Nov 17;17(11):e0277496. doi: 10.1371/journal.pone.0277496. eCollection 2022. PLoS One. 2022. PMID: 36395201 Free PMC article.
-
Breaking Bad News During Prenatal Screening: The Role of Professional Obstetricians and Midwives in Greece.Cureus. 2024 Mar 23;16(3):e56787. doi: 10.7759/cureus.56787. eCollection 2024 Mar. Cureus. 2024. PMID: 38650784 Free PMC article.
-
Breaking bad news in prenatal medicine: a literature review.J Reprod Infant Psychol. 2017 Feb;35(1):14-31. doi: 10.1080/02646838.2016.1253052. Epub 2016 Nov 22. J Reprod Infant Psychol. 2017. PMID: 29517292 Review.
-
[Are schizophrenic patients being told their diagnosis today in France?].Encephale. 2017 Apr;43(2):160-169. doi: 10.1016/j.encep.2016.01.011. Epub 2016 Jun 29. Encephale. 2017. PMID: 27372353 Review. French.
Cited by
-
Personality traits and stress coping among obstetricians diagnosing and communicating fetal death: A cross-sectional study.Int J Gynaecol Obstet. 2022 Aug;158(2):453-461. doi: 10.1002/ijgo.14048. Epub 2021 Dec 11. Int J Gynaecol Obstet. 2022. PMID: 34837223 Free PMC article.
References
-
- Korteweg F.J., Gordijn S.J., Timmer A., Erwich J.J., Bergman K.A., Bouman K., Ravise J.M., Heringa M.P., Holm J.P. The Tulip classification of perinatal mortality: Introduction and multidisciplinary inter-rater agreement. BJOG Int. J. Obstet. Gynaecol. 2006;113:393–401. doi: 10.1111/j.1471-0528.2006.00881.x. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
