

Practice Guidelines of the Central European Hepatologic Collaboration (CEHC) on the Use of Thrombopoietin Receptor Agonists in Patients with Chronic Liver Disease Undergoing Invasive Procedures
- PMID: 34830701
- PMCID: PMC8625449
- DOI: 10.3390/jcm10225419
Practice Guidelines of the Central European Hepatologic Collaboration (CEHC) on the Use of Thrombopoietin Receptor Agonists in Patients with Chronic Liver Disease Undergoing Invasive Procedures
Abstract
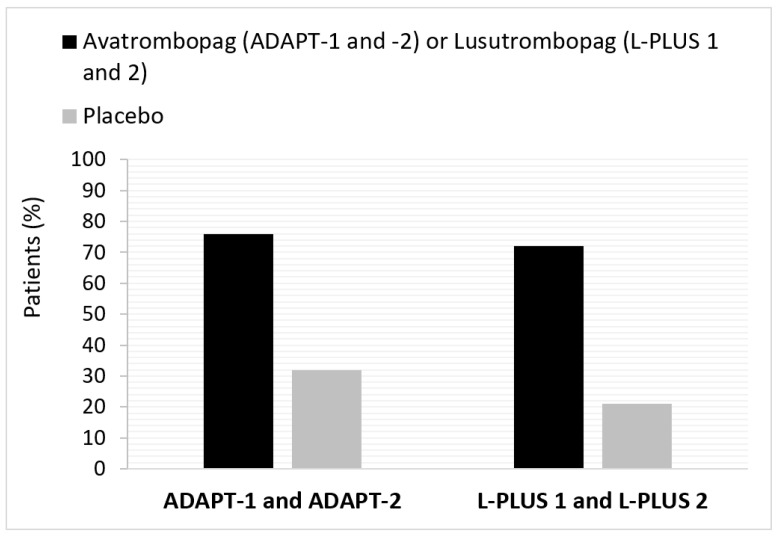
Background: Second-generation thrombopoietin receptor agonists (TPO-RAs) are emerging as the new standard for managing thrombocytopenia (TCP) in patients with chronic liver diseases (CLDs) undergoing scheduled procedures. However, practical guidance for their routine use in CLD patients undergoing specific invasive procedures is lacking.
Methods: These practice guidelines were developed by the Initiative Group for Central European Hepatologic Collaboration (CEHC), composed of nine hepatologist/gastroenterologist experts from Central Europe. Using an adapted Delphi process, the CEHC group selected ten invasive procedures most relevant to the hepatology/gastroenterology setting in the region. Consensus recommendations for each invasive procedure are reported as a final percentage of expert panel responses.
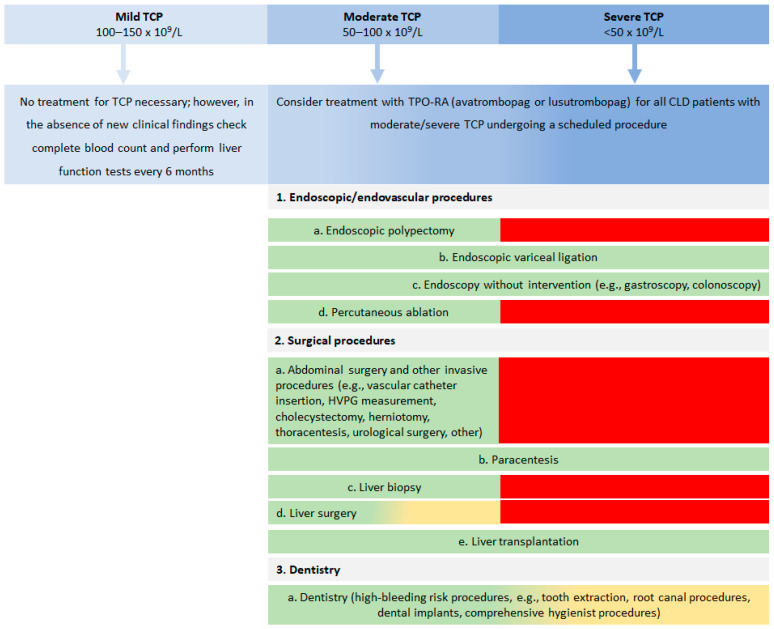
Results: A consensus was agreed that TPO-RAs should be considered for raising platelet count in CLD patients undergoing scheduled abdominal surgery, high-bleeding risk dentistry, endoscopic polypectomy, endoscopic variceal ligation, liver biopsy, liver surgery, liver transplantation and percutaneous ablation, but it was also agreed that they are less beneficial or not necessary for endoscopy without intervention and paracentesis.
Conclusions: Using a modified Delphi method, experts reached an agreement for TCP management in CLD patients undergoing ten invasive procedures. These practice guidelines may help with decision making and patient management in areas where clinical evidence is absent or limited.
Keywords: avatrombopag; chronic liver disease; platelet transfusion; surgical procedures; thrombocytopenia; thrombopoietin receptor agonists.
Conflict of interest statement
All authors declare no conflict of interest. The sponsor had no role in the collection, analyses, or interpretation of data in the writing of the manuscript or in the decision to publish the results.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
