

The Hepatic Sinusoid in Chronic Liver Disease: The Optimal Milieu for Cancer
- PMID: 34830874
- PMCID: PMC8616349
- DOI: 10.3390/cancers13225719
The Hepatic Sinusoid in Chronic Liver Disease: The Optimal Milieu for Cancer
Abstract
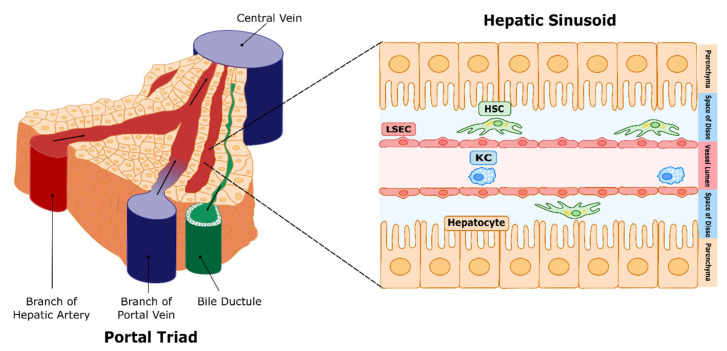
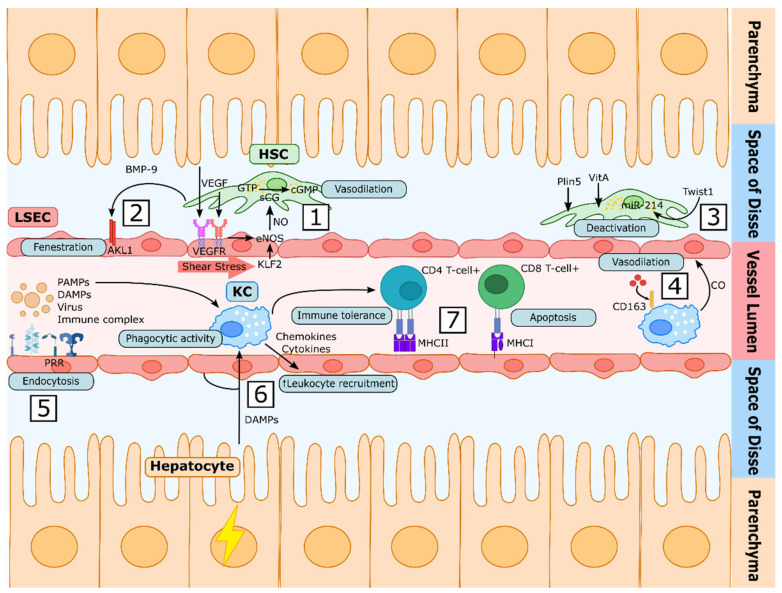
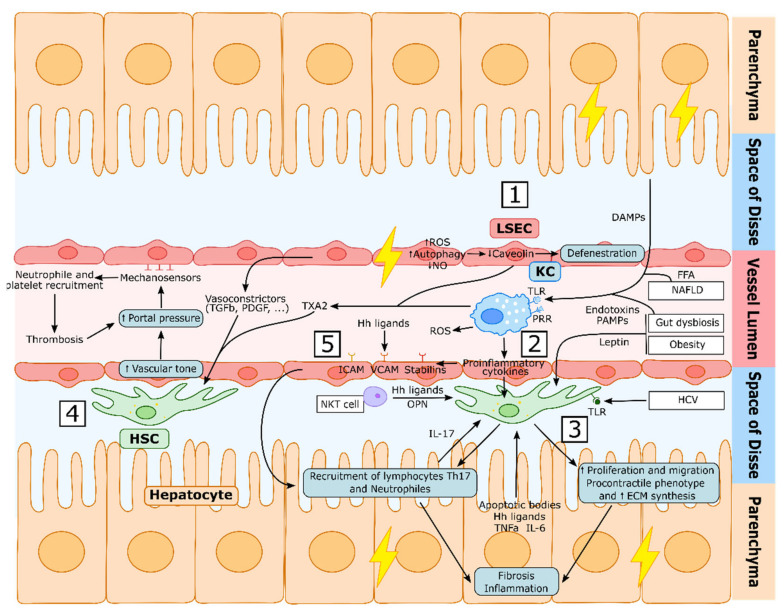
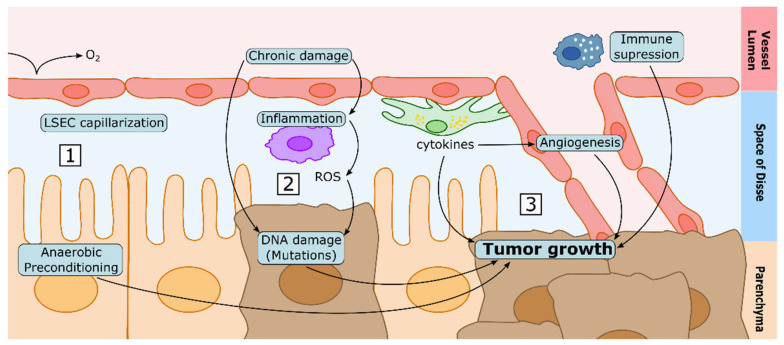
The liver sinusoids are a unique type of microvascular beds. The specialized phenotype of sinusoidal cells is essential for their communication, and for the function of all hepatic cell types, including hepatocytes. Liver sinusoidal endothelial cells (LSECs) conform the inner layer of the sinusoids, which is permeable due to the fenestrae across the cytoplasm; hepatic stellate cells (HSCs) surround LSECs, regulate the vascular tone, and synthetize the extracellular matrix, and Kupffer cells (KCs) are the liver-resident macrophages. Upon injury, the harmonic equilibrium in sinusoidal communication is disrupted, leading to phenotypic alterations that may affect the function of the whole liver if the damage persists. Understanding how the specialized sinusoidal cells work in coordination with each other in healthy livers and chronic liver disease is of the utmost importance for the discovery of new therapeutic targets and the design of novel pharmacological strategies. In this manuscript, we summarize the current knowledge on the role of sinusoidal cells and their communication both in health and chronic liver diseases, and their potential pharmacologic modulation. Finally, we discuss how alterations occurring during chronic injury may contribute to the development of hepatocellular carcinoma, which is usually developed in the background of chronic liver disease.
Keywords: CLD; HSC; Kupffer cell; LSEC; NASH; cirrhosis; hepatocellular carcinoma; portal hypertension.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
