

Interstitial Photodynamic Therapy for Glioblastomas: A Standardized Procedure for Clinical Use
- PMID: 34830908
- PMCID: PMC8616201
- DOI: 10.3390/cancers13225754
Interstitial Photodynamic Therapy for Glioblastomas: A Standardized Procedure for Clinical Use
Abstract
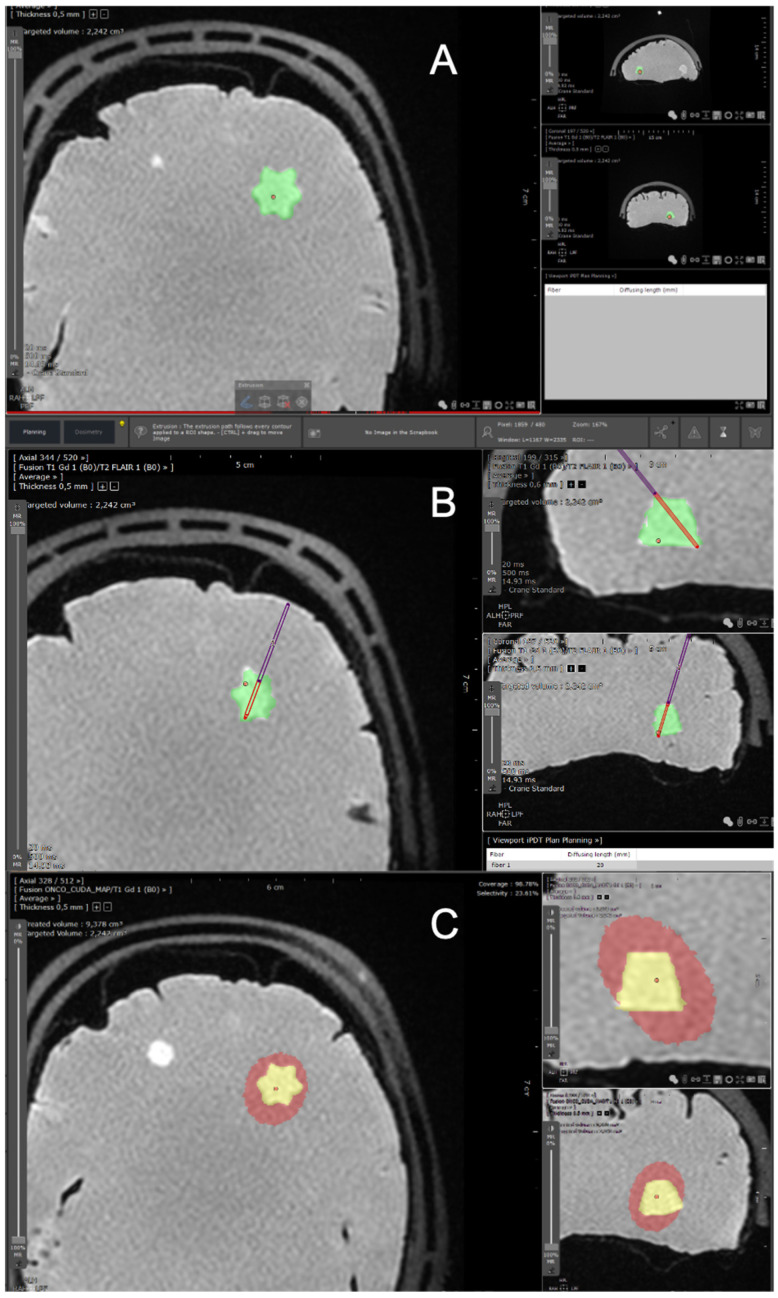
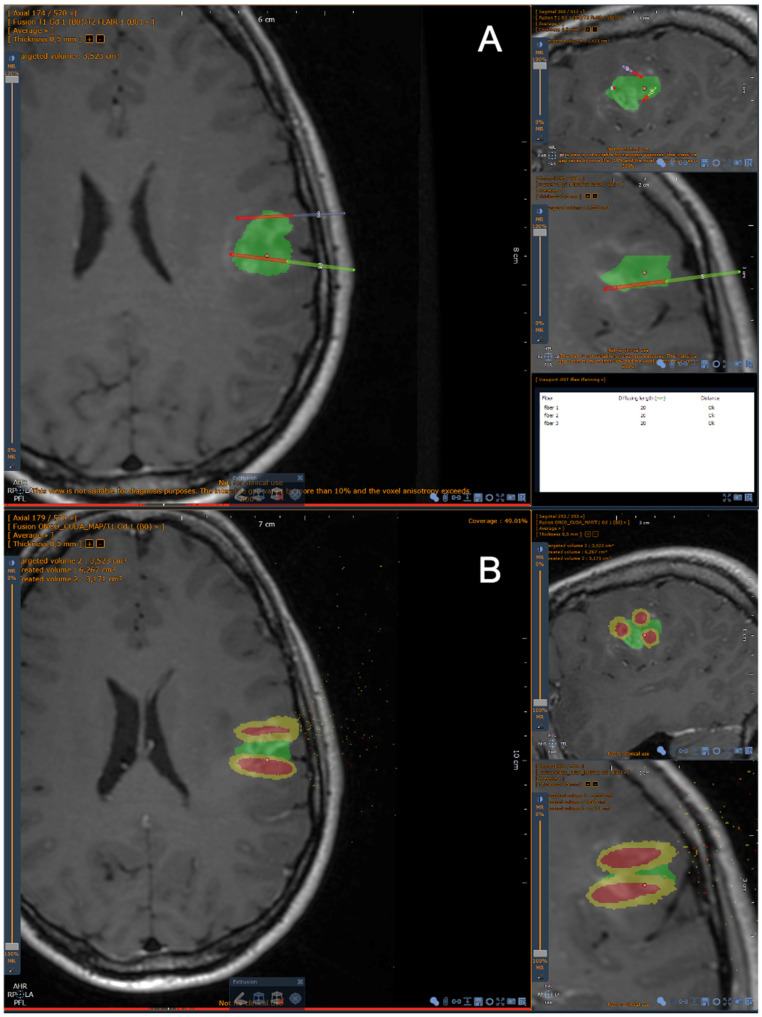
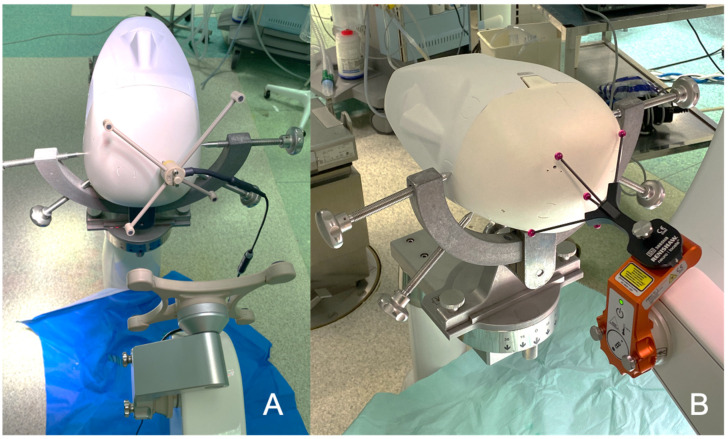
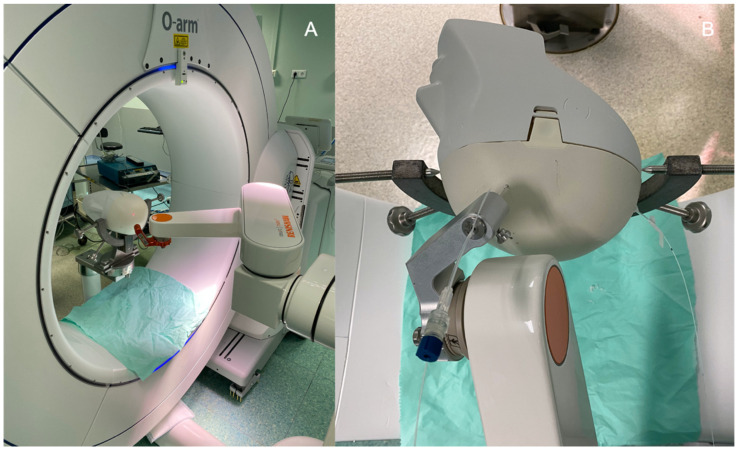
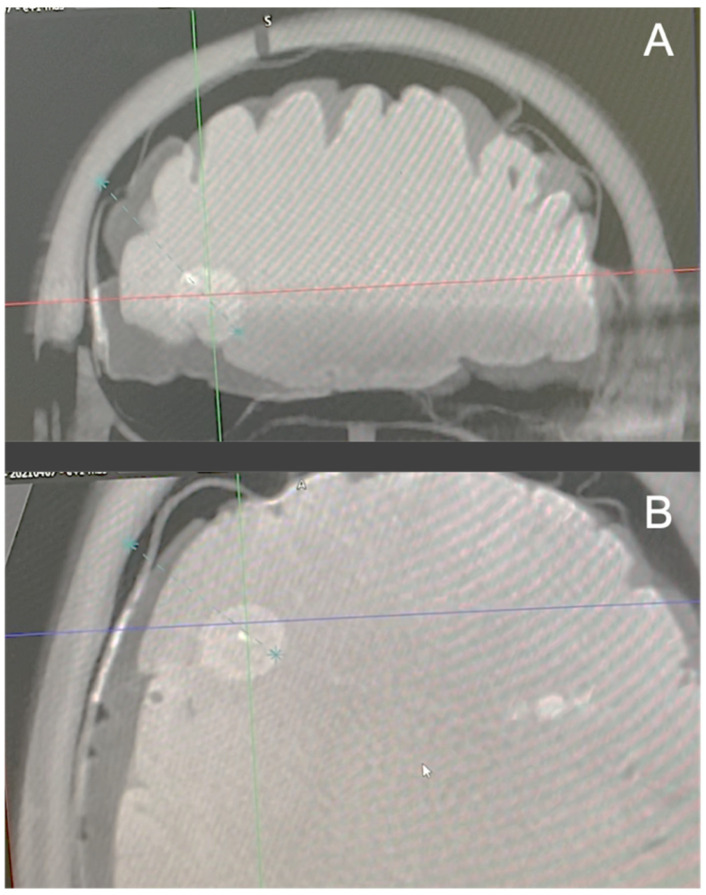
Glioblastomas (GBMs) are high-grade malignancies with a poor prognosis. The current standard of care for GBM is maximal surgical resection followed by radiotherapy and chemotherapy. Despite all these treatments, the overall survival is still limited, with a median of 15 months. For patients harboring inoperable GBM, due to the anatomical location of the tumor or poor general condition of the patient, the life expectancy is even worse. The challenge of managing GBM is therefore to improve the local control especially for non-surgical patients. Interstitial photodynamic therapy (iPDT) is a minimally invasive treatment relying on the interaction of light, a photosensitizer and oxygen. In the case of brain tumors, iPDT consists of introducing one or several optical fibers in the tumor area, without large craniotomy, to illuminate the photosensitized tumor cells. It induces necrosis and/or apoptosis of the tumor cells, and it can destruct the tumor vasculature and produces an acute inflammatory response that attracts leukocytes. Interstitial PDT has already been applied in the treatment of brain tumors with very promising results. However, no standardized procedure has emerged from previous studies. Herein, we propose a standardized and reproducible workflow for the clinical application of iPDT to GBM. This workflow, which involves intraoperative imaging, a dedicated treatment planning system (TPS) and robotic assistance for the implantation of stereotactic optical fibers, represents a key step in the deployment of iPDT for the treatment of GBM. This end-to-end procedure has been validated on a phantom in real operating room conditions. The thorough description of a fully integrated iPDT workflow is an essential step forward to a clinical trial to evaluate iPDT in the treatment of GBM.
Keywords: brain tumor; glioblastoma; interstitial; photodynamic therapy; treatment planning system.
Conflict of interest statement
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Figures
Similar articles
-
Interstitial photodynamic therapy for newly diagnosed glioblastoma.J Neurooncol. 2023 Mar;162(1):217-223. doi: 10.1007/s11060-023-04284-9. Epub 2023 Mar 16. J Neurooncol. 2023. PMID: 36928699 Free PMC article.
-
Interstitial Photodynamic Therapy of Glioblastomas: A Long-Term Follow-up Analysis of Survival and Volumetric MRI Data.Cancers (Basel). 2023 May 4;15(9):2603. doi: 10.3390/cancers15092603. Cancers (Basel). 2023. PMID: 37174068 Free PMC article.
-
Interrelation between Spectral Online Monitoring and Postoperative T1-Weighted MRI in Interstitial Photodynamic Therapy of Malignant Gliomas.Cancers (Basel). 2021 Dec 27;14(1):120. doi: 10.3390/cancers14010120. Cancers (Basel). 2021. PMID: 35008284 Free PMC article.
-
Nanomedicine in Clinical Photodynamic Therapy for the Treatment of Brain Tumors.Biomedicines. 2022 Jan 3;10(1):96. doi: 10.3390/biomedicines10010096. Biomedicines. 2022. PMID: 35052776 Free PMC article. Review.
-
Nanomedicine associated with photodynamic therapy for glioblastoma treatment.Biophys Rev. 2017 Oct;9(5):761-773. doi: 10.1007/s12551-017-0293-3. Epub 2017 Aug 19. Biophys Rev. 2017. PMID: 28823025 Free PMC article. Review.
Cited by
-
Long term follow-up of patients with newly diagnosed glioblastoma treated by intraoperative photodynamic therapy: an update from the INDYGO trial (NCT03048240).J Neurooncol. 2024 Jul;168(3):495-505. doi: 10.1007/s11060-024-04693-4. Epub 2024 May 16. J Neurooncol. 2024. PMID: 38753093 Free PMC article.
-
Preclinical Studies with Glioblastoma Brain Organoid Co-Cultures Show Efficient 5-ALA Photodynamic Therapy.Cells. 2023 Apr 10;12(8):1125. doi: 10.3390/cells12081125. Cells. 2023. PMID: 37190034 Free PMC article.
-
Precision Killing of Sinoporphyrin Sodium-Mediated Photodynamic Therapy against Malignant Tumor Cells.Int J Mol Sci. 2022 Sep 12;23(18):10561. doi: 10.3390/ijms231810561. Int J Mol Sci. 2022. PMID: 36142474 Free PMC article.
-
Photodynamic therapy and tumor-treating fields therapy for newly diagnosed glioblastoma.Front Oncol. 2025 Feb 28;15:1556669. doi: 10.3389/fonc.2025.1556669. eCollection 2025. Front Oncol. 2025. PMID: 40094018 Free PMC article.
-
Photodynamic opening of the blood-brain barrier affects meningeal lymphatics and the brain's drainage in healthy male mice.Biomed Opt Express. 2024 Sep 26;15(10):6063-6072. doi: 10.1364/BOE.527892. eCollection 2024 Oct 1. Biomed Opt Express. 2024. PMID: 39421760 Free PMC article.
References
-
- McGirt M.J., Chaichana K.L., Gathinji M., Attenello F.J., Than K., Olivi A., Weingart J.D., Brem H., Quiñones-Hinojosa A. redo Independent Association of Extent of Resection with Survival in Patients with Malignant Brain Astrocytoma: Clinical Article. J. Neurosurg. 2009;110:156–162. doi: 10.3171/2008.4.17536. - DOI - PubMed
-
- Stummer W., Pichlmeier U., Meinel T., Wiestler O.D., Zanella F., Reulen H.-J., ALA-Glioma Study Group Fluorescence-Guided Surgery with 5-Aminolevulinic Acid for Resection of Malignant Glioma: A Randomised Controlled Multicentre Phase III Trial. Lancet Oncol. 2006;7:392–401. doi: 10.1016/S1470-2045(06)70665-9. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
