

Tylectomy Safety in Salvage of Eyes with Retinoblastoma
- PMID: 34831013
- PMCID: PMC8616183
- DOI: 10.3390/cancers13225862
Tylectomy Safety in Salvage of Eyes with Retinoblastoma
Abstract
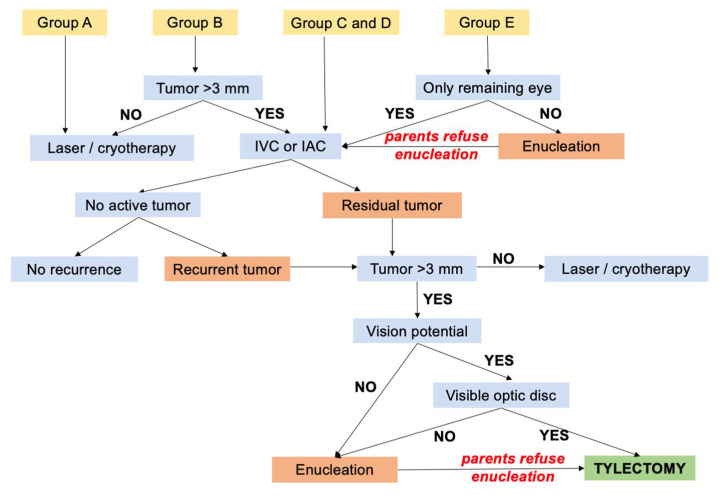
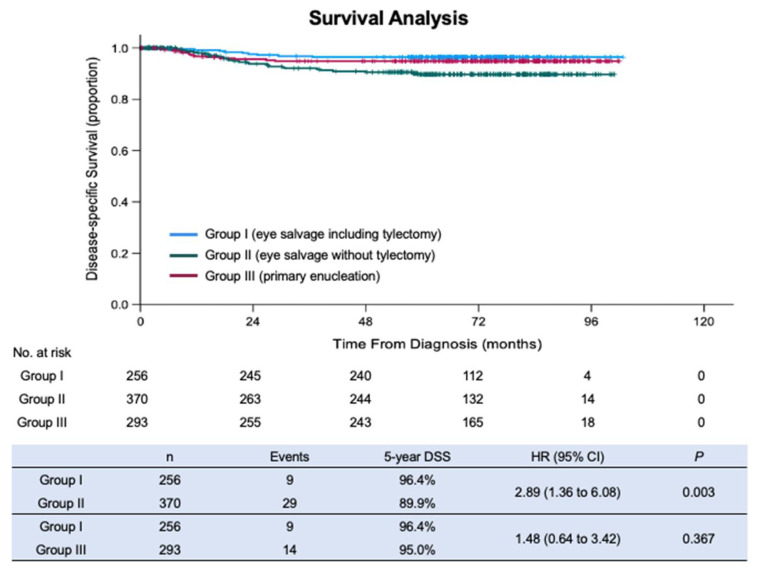
Intraocular surgery is tabooed in retinoblastoma management, due to the concern of lethal extraocular spread. We reviewed the outcomes of consecutive children with intraocular retinoblastoma diagnosed at 29 Chinese centers between 2012-2014. We compared the outcomes of three categories of treatment: eye salvage including tylectomy (Group I), eye salvage without tylectomy (Group II), and primary enucleation (Group III). A total of 960 patients (1243 eyes) were diagnosed: 256 in Group I, 370 in Group II, and 293 in Group III; 41 patients abandoned treatment upfront. The estimated 5-year overall survivals (OS) were, for Group I, 94%, for Group II 89%, and for Group III 95%. The estimated 5-year disease-specific survivals (DSS) were, for Group I, 96%, for Group II 90%, and for Group III 95%. Patients in Group I had a significantly higher 5-year DSS than patients in Group II (p = 0.003) and not significantly different than patients in Group III (p = 0.367). Overall survival was not compromised by the inclusion of tylectomy in eye salvage therapy compared to eye salvage without tylectomy or primary enucleation. Disease-specific survival was better when tylectomy was included in eye salvage treatments. Tylectomy as part of multimodal treatment may contribute to the care of retinoblastoma patients with chemotherapy-resistant tumor, eyes with concomitant ocular complications, or at the risk of treatment abandonment.
Keywords: endoresection; enucleation; pars plana vitrectomy; resection; retinoblastoma; safety; surgery; survival; tylectomy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Francis J.H., Abramson D.H., Ji X., Shields C.L., Teixeira L.F., Schefler A.C., Cassoux N., Hadjistilianou D., Berry J.L., Frenkel S., et al. Risk of Extraocular Extension in Eyes With Retinoblastoma Receiving Intravitreous Chemotherapy. JAMA Ophthalmol. 2017;135:1426–1429. doi: 10.1001/jamaophthalmol.2017.4600. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
