

Expanding the Evidence of a Semi-Dominant Inheritance in GDF2 Associated with Pulmonary Arterial Hypertension
- PMID: 34831401
- PMCID: PMC8624726
- DOI: 10.3390/cells10113178
Expanding the Evidence of a Semi-Dominant Inheritance in GDF2 Associated with Pulmonary Arterial Hypertension
Abstract
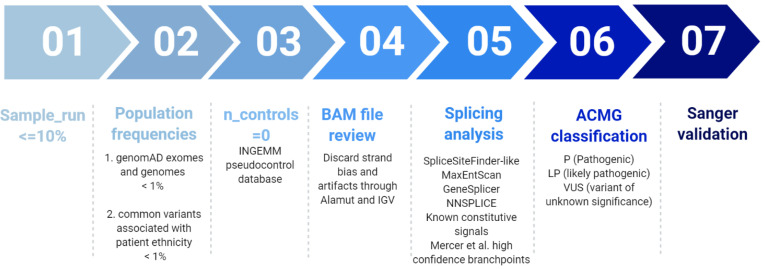
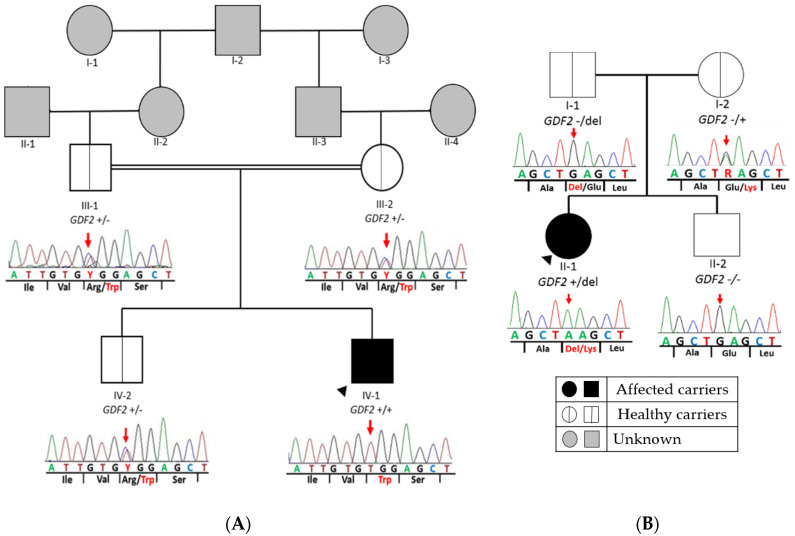
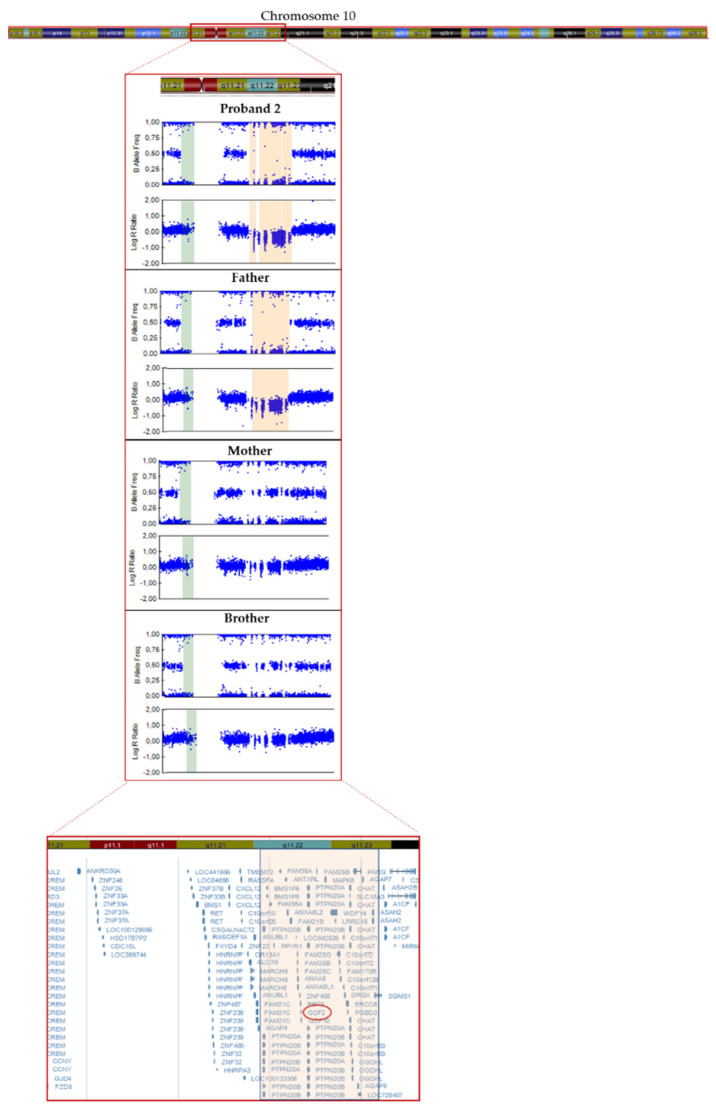
Pulmonary arterial hypertension (PAH) sometimes co-exists with hereditary hemorrhagic telangiectasia (HHT). Despite being clinically diagnosable according to Curaçao criteria, HHT can be difficult to diagnose due to its clinically heterogenicity and highly overlapping with PAH. Genetic analysis of the associated genes ACVRL1, ENG, SMAD4 and GDF2 can help to confirm or discard the presumptive diagnosis. As part of the clinical routine and to establish a genetic diagnosis, we have analyzed a cohort of patients with PAH and overlapping HHT features through a customized Next Generation Sequencing (NGS) panel of 21 genes, designed and validated in-house. We detected a homozygous missense variant in GDF2 in a pediatric patient diagnosed with PAH associated with HHT and a missense variant along with a heterozygous deletion in another idiopathic PAH patient (compound heterozygous inheritance). In order to establish variant segregation, we analyzed all available family members. In both cases, parents were carriers for the variants, but neither was affected. Our results expand the clinical spectrum and the inheritance pattern associated with GDF2 pathogenic variants suggesting incomplete penetrance and/or variability of expressivity with a semi-dominant pattern of inheritance.
Keywords: GDF2; NGS; genomic medicine; hereditary hemorrhagic telangiectasia; massive parallel sequencing; personalized medicine; pulmonary arterial hypertension.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Galiè N., Humbert M., Vachiery J., Gibbs S., Lang I., Torbicki A., Simonneau G., Peacock A., Vonk Noordegraaf A., Beghetti M. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT) Eur. Heart J. 2016;37:67–119. - PubMed
-
- Deng Z., Morse J.H., Slager S.L., Cuervo N., Moore K.J., Venetos G., Kalachikov S., Cayanis E., Fischer S.G., Barst R.J. Familial primary pulmonary hypertension (Gene PPH1) is caused by mutations in the bone morphogenetic protein receptor–II gene. Am. J. Hum. Genet. 2000;67:737–744. doi: 10.1086/303059. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
