

Clostridioides difficile and Vancomycin-Resistant Enterococci in COVID-19 Patients with Severe Pneumonia
- PMID: 34833003
- PMCID: PMC8653967
- DOI: 10.3390/life11111127
Clostridioides difficile and Vancomycin-Resistant Enterococci in COVID-19 Patients with Severe Pneumonia
Abstract
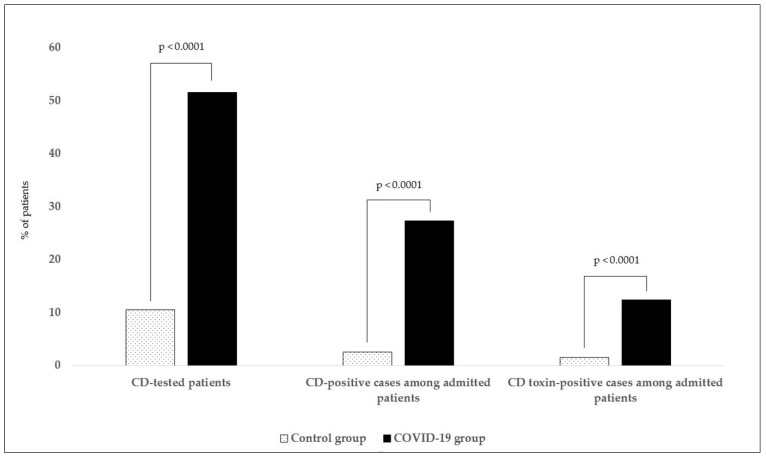
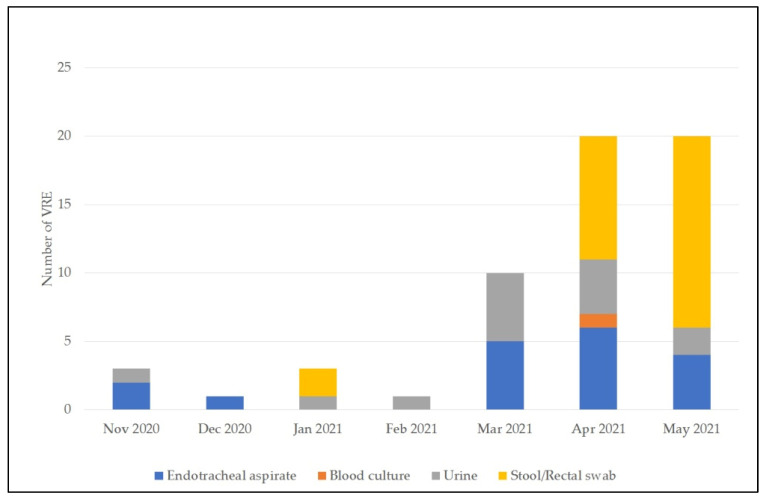
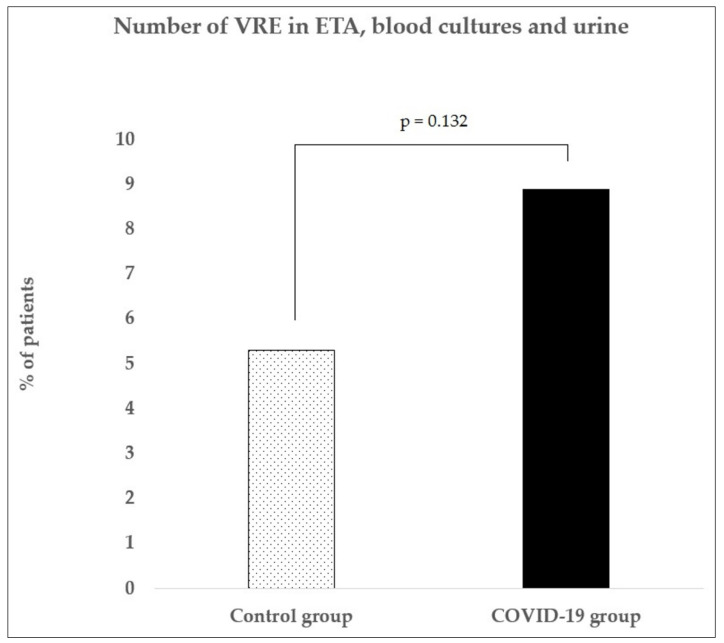
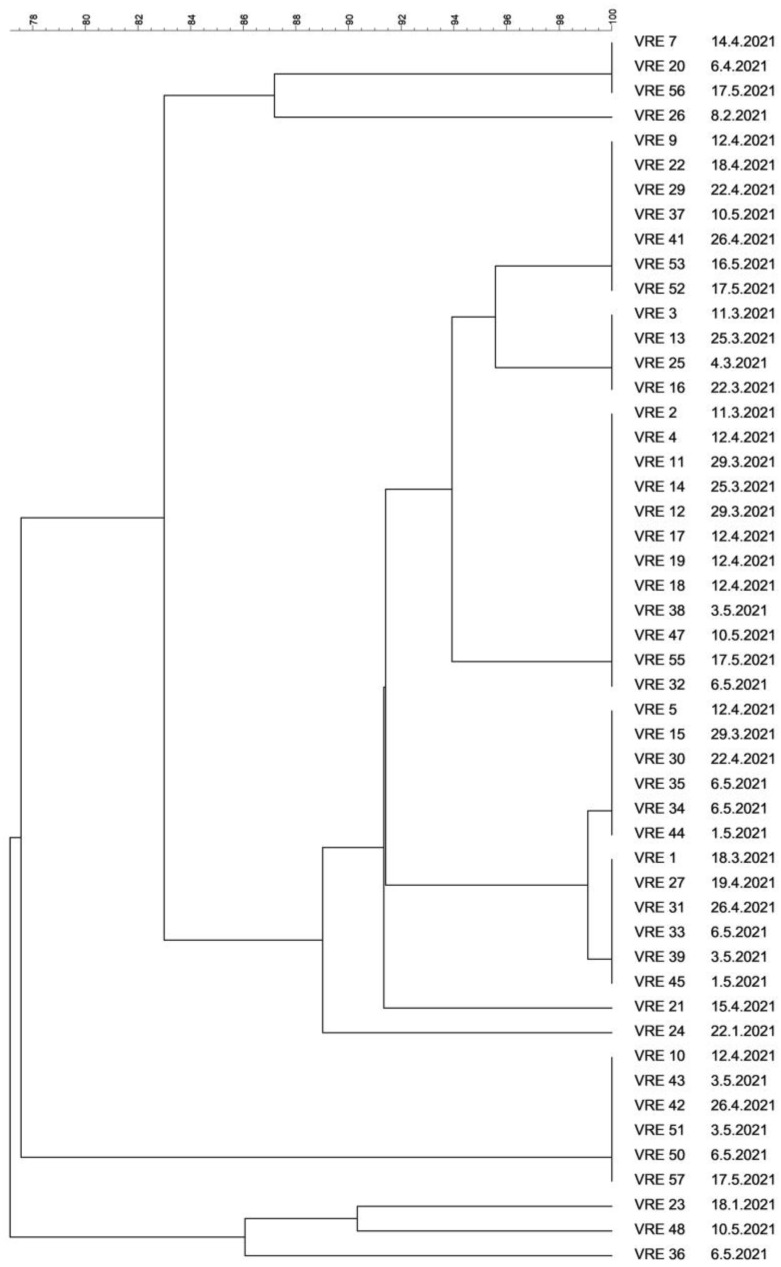
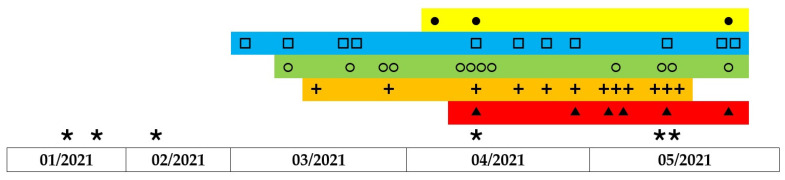
Broad-spectrum antibiotics administered to patients with severe COVID-19 pneumonia pose a risk of infection caused by Clostridioides difficile. This risk is reduced mainly by strict hygiene measures and early de-escalation of antibiotic therapy. Recently, oral vancomycin prophylaxis (OVP) has also been discussed. This retrospective study aimed to assess the prevalence of C. difficile in critical COVID-19 patients staying in an intensive care unit of a tertiary hospital department of anesthesiology, resuscitation, and intensive care from November 2020 to May 2021 and the rates of vancomycin-resistant enterococci (VRE) after the introduction of OVP and to compare the data with those from controls in the pre-pandemic period (November 2018 to May 2019). During the COVID-19 pandemic, there was a significant increase in toxigenic C. difficile rates to 12.4% of patients, as compared with 1.6% in controls. The peak rates were noted in February 2021 (25% of patients), immediately followed by initiation of OVP, changes to hygiene precautions, and more rapid de-escalation of antibiotic therapy. Subsequently, toxigenic C. difficile detection rates started to fall. There was a nonsignificant increase in VRE detected in non-gastrointestinal tract samples to 8.9% in the COVID-19 group, as compared to 5.3% in the control group. Molecular analysis confirmed mainly clonal spread of VRE.
Keywords: COVID-19; Clostridioides difficile; ICU; molecular typing of VRE; oral vancomycin prophylaxis; vancomycin-resistant enterococci.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- World Health Organization Clinical Management of COVID-19: Interim Guidance, 27 May 2020. [(accessed on 29 August 2021)]. Available online: https://apps.who.int/iris/handle/10665/332196.
-
- Martín-Loeches I., Sanchez-Corral A., Diaz E., Granada R., Zaragoza R., Villavicencio C., Albaya A., Cerdá E., Catalán R., Luque P., et al. Community-Acquired Respiratory Coinfection in Critically Ill Patients with Pandemic 2009 Influenza A(H1N1) Virus. Chest. 2011;139:555–562. doi: 10.1378/chest.10-1396. - DOI - PubMed
-
- Ponce-Alonso M., Sáez de la Fuente J., Rincón-Carlavilla A., Moreno-Nunez P., Martínez-García L., Escudero-Sánchez R., Pintor R., García-Fernández S., Cobo J. Impact of the coronavirus disease 2019 (COVID-19) pandemic on nosocomial Clostridioides difficile infection. Infect. Control. Hosp. Epidemiol. 2021;42:406–410. doi: 10.1017/ice.2020.454. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
