

Genital Lymphedema and How to Deal with It: Pearls and Pitfalls from over 38 Years of Experience with Unusual Lymphatic System Impairment
- PMID: 34833393
- PMCID: PMC8618468
- DOI: 10.3390/medicina57111175
Genital Lymphedema and How to Deal with It: Pearls and Pitfalls from over 38 Years of Experience with Unusual Lymphatic System Impairment
Abstract
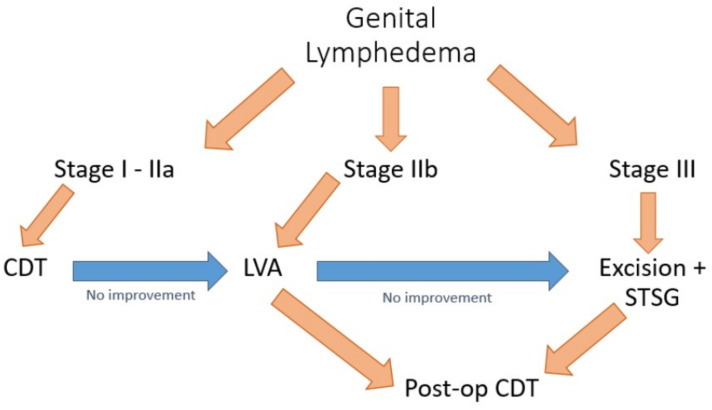
Background and Objectives: Conservative treatment represents an essential pillar of lymphedema management, along with debulking and physiologic surgeries. Despite the consistent number of treatment options, there is currently no agreement on their indications and possible combinations. When dealing with unusual lymphedema presentation as in the genitalia (Genital Lymphedema-GL), treatment choice becomes even more difficult. The authors aimed to present their targeted algorithm of single and combined treatment modalities for rare GL in order to face this paucity of information. Materials and Methods: Data were collected from a prospectively maintained database since January 1983, and cases of GL that were managed in the authors' department were selected. Only patients that were treated in the authors' institution and presented a minimum follow-up of 3 months were admitted to the current study. Results: From January 1983 to July 2021, 19 patients with GL were recruited. All the patients were male, and their ages ranged from 21 to 73 years old (average: 52). Ten cases (52.6%) presented with ISL (International Society of Lymphology) stage I, five (26.3%) were stage II and four (21.1%) were stage III. GL was managed with conservative treatment (12 cases), LVA (LymphaticoVenous Anastomosis) (3) or surgical excision (4). In a mean follow-up of 7.5 years (range: 3 months-11 years), no major complications occurred, and all cases reached improvements in functional and quality of life terms. Conclusions: Contrary to the predominant thought of the necessity to avoid surgery in unusual lymphedema presentations such as GL, they can be managed using targeted multimodal approaches or by adapting well-known procedures in unusual ways to achieve control of disease progression and improve patients' quality of life.
Keywords: debulking surgery; genital lymphedema; multimodal approach; physiologic surgery; rare lymphedema; targeted therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Lymphovenous anastomosis and debulking procedure for treatment of combined severe lower extremity and genital lymphedema: A case report.Microsurgery. 2018 Nov;38(8):907-911. doi: 10.1002/micr.30331. Epub 2018 May 2. Microsurgery. 2018. PMID: 29719080
-
A Systematic Review of Outcomes After Genital Lymphedema Surgery: Microsurgical Reconstruction Versus Excisional Procedures.Ann Plast Surg. 2019 Dec;83(6):e85-e91. doi: 10.1097/SAP.0000000000001875. Ann Plast Surg. 2019. PMID: 31135508
-
Lymphatic venous anastomosis (LVA) for treatment of secondary arm lymphedema. A prospective study of 11 LVA procedures in 10 patients with breast cancer related lymphedema and a critical review of the literature.Breast Cancer Res Treat. 2009 Jan;113(2):199-206. doi: 10.1007/s10549-008-9932-5. Epub 2008 Feb 13. Breast Cancer Res Treat. 2009. PMID: 18270813 Review.
-
Lymphedema surgery: the current state of the art.Clin Exp Metastasis. 2018 Aug;35(5-6):553-558. doi: 10.1007/s10585-018-9897-7. Epub 2018 Jul 6. Clin Exp Metastasis. 2018. PMID: 29980891
-
The utility of surgical and conservative combination therapy for advanced stage lymphedema.J Vasc Surg Venous Lymphat Disord. 2021 Jan;9(1):234-241. doi: 10.1016/j.jvsv.2020.05.007. Epub 2020 May 26. J Vasc Surg Venous Lymphat Disord. 2021. PMID: 32470619
Cited by
-
Distally Prophylactic Lymphaticovenular Anastomoses after Axillary or Inguinal Complete Lymph Node Dissection Followed by Radiotherapy: A Case Series.Medicina (Kaunas). 2022 Jan 29;58(2):207. doi: 10.3390/medicina58020207. Medicina (Kaunas). 2022. PMID: 35208531 Free PMC article.
-
Surgical Treatment and Rehabilitation Strategies for Upper and Lower Extremity Lymphedema: A Comprehensive Review.Medicina (Kaunas). 2022 Jul 19;58(7):954. doi: 10.3390/medicina58070954. Medicina (Kaunas). 2022. PMID: 35888673 Free PMC article. Review.
-
Surgical Applications of Lymphatic Vessel Visualization Using Photoacoustic Imaging and Augmented Reality.J Clin Med. 2021 Dec 30;11(1):194. doi: 10.3390/jcm11010194. J Clin Med. 2021. PMID: 35011933 Free PMC article.
-
Combination of conservative and surgical methods in the treatment of giant lymphedema of the scrotum: A case report.Front Surg. 2023 Apr 12;10:1048159. doi: 10.3389/fsurg.2023.1048159. eCollection 2023. Front Surg. 2023. PMID: 37123541 Free PMC article.
-
Concordance between preoperative imaging methods in patients with limb lymphedema undergoing supermicrosurgical lymphaticovenular anastomosis.J Vasc Surg Venous Lymphat Disord. 2024 Nov;12(6):101891. doi: 10.1016/j.jvsv.2024.101891. Epub 2024 Apr 15. J Vasc Surg Venous Lymphat Disord. 2024. PMID: 38631506 Free PMC article.
References
-
- Szuba A., Shin W.S., Strauss H.W., Rockson S. The third circulation: Radionuclide lymphoscintigraphy in the evaluation of lymphedema. J. Nucl. Med. 2003;44:43–57. - PubMed
-
- Corum M., Basoglu C., Korkmaz M.D., Yildirim M.A., Ones K. Effectiveness of Combined Complex Decongestive Therapy and Resistance Exercises in the Treatment of Lymphedema Associated with Breast Cancer and the Effect of Pain on Treatment Response. Lymphat. Res. Biol. 2021;19:383–390. doi: 10.1089/lrb.2020.0099. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
