

Role of Photobiomodulation Therapy in Neurological Primary Burning Mouth Syndrome. A Systematic Review and Meta-Analysis of Human Randomised Controlled Clinical Trials
- PMID: 34834253
- PMCID: PMC8624276
- DOI: 10.3390/pharmaceutics13111838
Role of Photobiomodulation Therapy in Neurological Primary Burning Mouth Syndrome. A Systematic Review and Meta-Analysis of Human Randomised Controlled Clinical Trials
Abstract
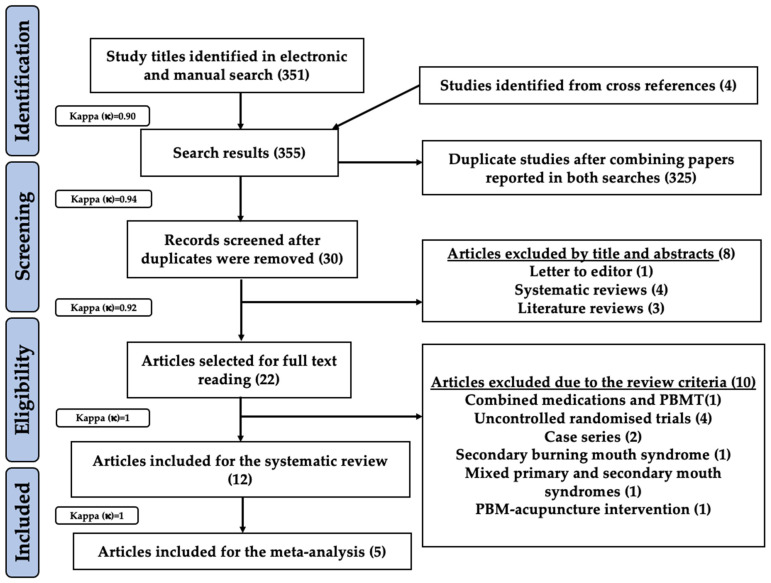
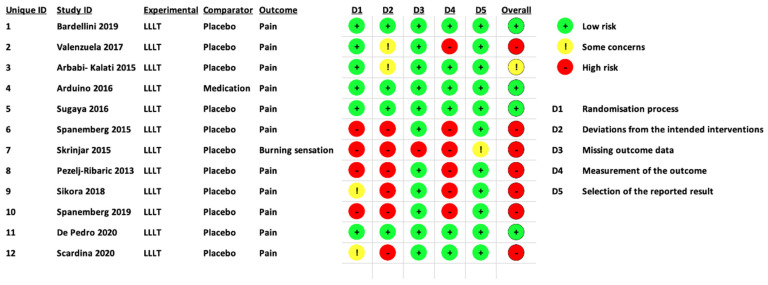
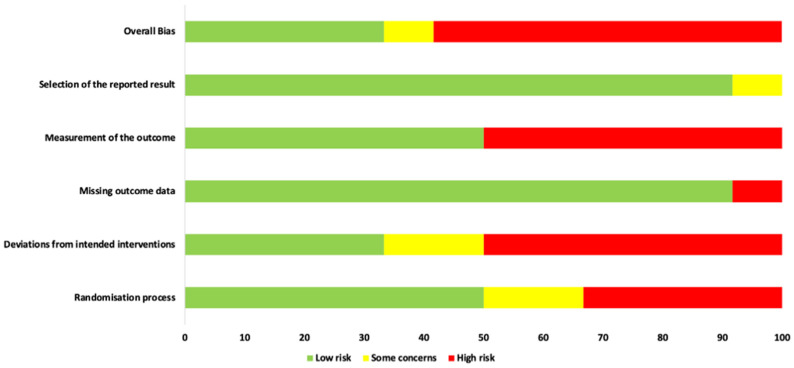
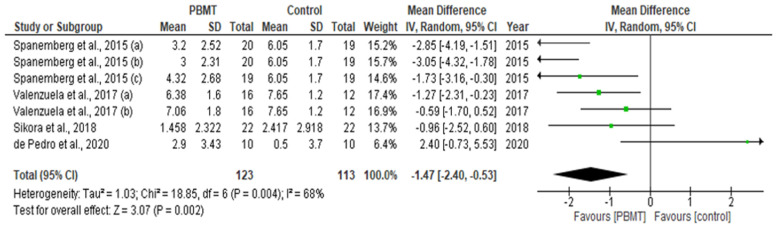
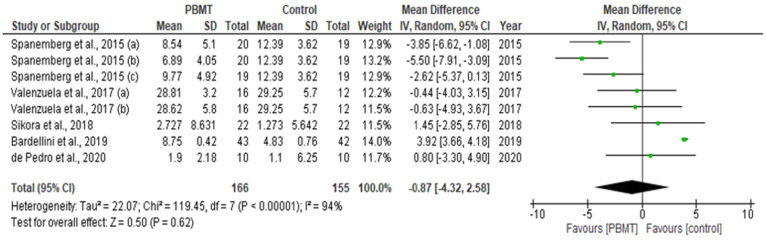
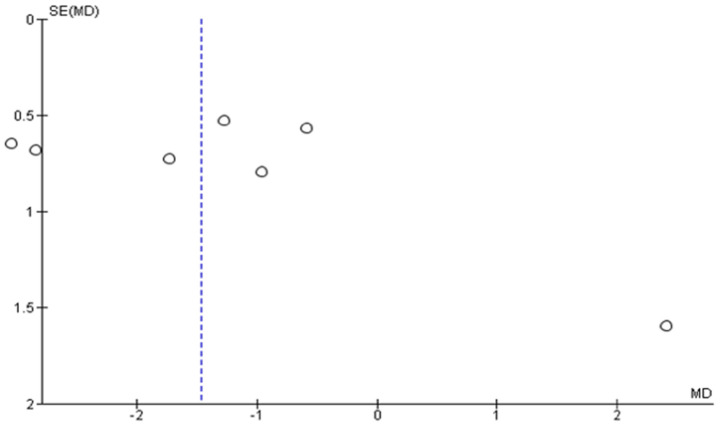
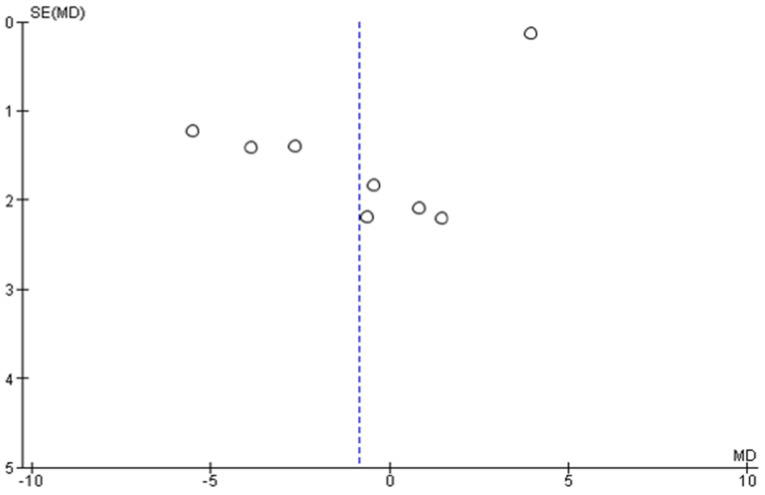
Mitochondrial homeostasis is crucial for energy production and neuronal survival in neurological primary burning mouth syndrome (npBMS). Photobiomodulation therapy (PBMT) has been utilised in npBMS management, however, its role of intervention remains controversial. The aim of this systematic review and meta-analysis of CRD 42020198921 PROSPERO registration reference was to oversee and determine the efficacy of PBMT in patients with npBMS, identifying the gaps and bridge them by proposing recommendations for future studies purposes. PRISMA guidelines and Cochrane Collaboration recommendations followed. Various search engines employed to analyse a total of 351 studies of which 12 were included. A wide range of utilised PBM wavelengths was between 635-980 nm and the power output ranged between 30 mW and 4000 mW. A high risk of bias (RoB) was noted in 7 out of 12 included studies (58.3%), as results of qualitative analysis. Meta-analysis findings of 4 out of 12 studies showed statistically significant intergroup differences (SSID) for visual analogue scale (VAS) values (MD = -1.47; 95% CI = -2.40 to -0.53; Z = 3.07 (p = 0.002) whereas meta-analysis on 5 out of 12 studies revealed SSID for anxiety/depression and quality of life (MD = -1.47; 95% CI = -2.40 to -0.53; Z = 3.07 (p = 0.002), favouring PBMT group to the control treatment strategies. Despite the inconsistency and diversity in PBM parameters (wavelength, power, light source, spot size, emission mode, energy per point, total energy) and treatment protocols (exposure time, number of sessions, time interval between sessions, treatment duration)-majority of the included studies showed positive PBM results. The high RoB and meta-analytical heterogeneity in the eligible studies warrant the necessity to perform well-designed and robust RCTs after acknowledging the drawbacks of the available scientific literature and addressing our suggested recommendations highlighted in our review.
Keywords: RCT; mitochondrial homeostasis; molecular mechanisms; neuropathic pain; outcome measures; oxidative stress; photobiomodulation; primary burning mouth syndrome; transmucosal; trigeminal nerve inflammation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Woda A., Navez M.L., Picard P., Gremeau C., Pichard-Leandri E. A possible therapeutic solution for stomatodynia (burning mouth syndrome) J. Orofac. Pain. 1998;12:272–278. - PubMed
-
- Merskey H., Bogduk N. Classification of Chronic Pain. International Association for the Study of Pain Press; Seattle, WA, USA: 1994. pp. 209–214.
Publication types
LinkOut - more resources
Full Text Sources
