

An Artificial Intelligence-Based Alarm Strategy Facilitates Management of Acute Myocardial Infarction
- PMID: 34834501
- PMCID: PMC8623357
- DOI: 10.3390/jpm11111149
An Artificial Intelligence-Based Alarm Strategy Facilitates Management of Acute Myocardial Infarction
Abstract
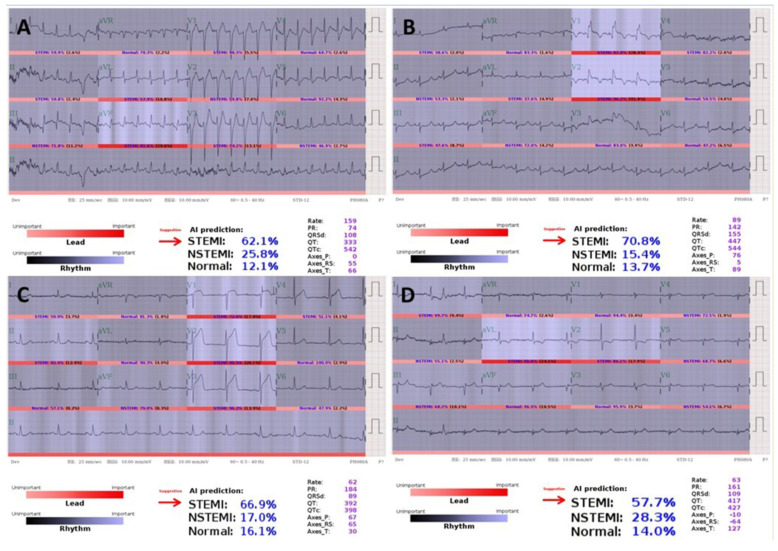
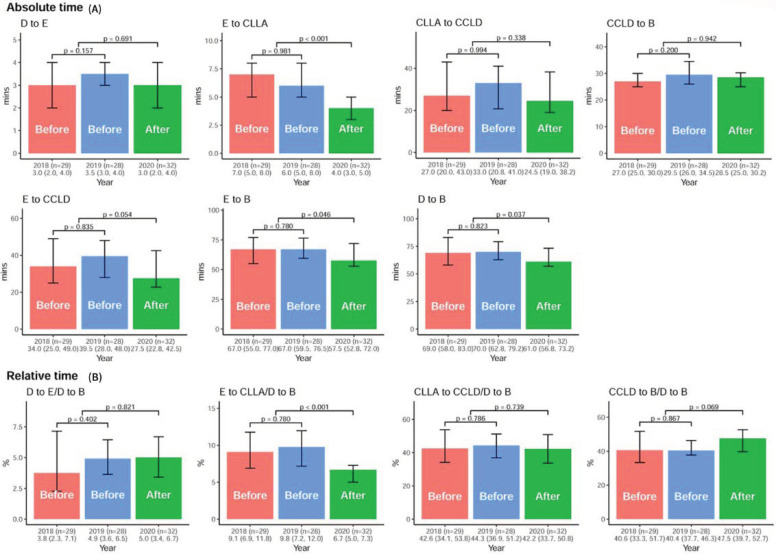
(1) Background: While an artificial intelligence (AI)-based, cardiologist-level, deep-learning model for detecting acute myocardial infarction (AMI), based on a 12-lead electrocardiogram (ECG), has been established to have extraordinary capabilities, its real-world performance and clinical applications are currently unknown. (2) Methods and Results: To set up an artificial intelligence-based alarm strategy (AI-S) for detecting AMI, we assembled a strategy development cohort including 25,002 visits from August 2019 to April 2020 and a prospective validation cohort including 14,296 visits from May to August 2020 at an emergency department. The components of AI-S consisted of chest pain symptoms, a 12-lead ECG, and high-sensitivity troponin I. The primary endpoint was to assess the performance of AI-S in the prospective validation cohort by evaluating F-measure, precision, and recall. The secondary endpoint was to evaluate the impact on door-to-balloon (DtoB) time before and after AI-S implementation in STEMI patients treated with primary percutaneous coronary intervention (PPCI). Patients with STEMI were alerted precisely by AI-S (F-measure = 0.932, precision of 93.2%, recall of 93.2%). Strikingly, in comparison with pre-AI-S (N = 57) and post-AI-S (N = 32) implantation in STEMI protocol, the median ECG-to-cardiac catheterization laboratory activation (EtoCCLA) time was significantly reduced from 6.0 (IQR, 5.0-8.0 min) to 4.0 min (IQR, 3.0-5.0 min) (p < 0.01). The median DtoB time was shortened from 69 (IQR, 61.0-82.0 min) to 61 min (IQR, 56.8-73.2 min) (p = 0.037). (3) Conclusions: AI-S offers front-line physicians a timely and reliable diagnostic decision-support system, thereby significantly reducing EtoCCLA and DtoB time, and facilitating the PPCI process. Nevertheless, large-scale, multi-institute, prospective, or randomized control studies are necessary to further confirm its real-world performance.
Keywords: acute myocardial infarction; alarm system; artificial intelligence; deep learning; electrocardiogram.
Conflict of interest statement
Authors declare no conflict of interest.
Figures



References
-
- Ibanez B., James S., Agewall S., Antunes M.J., Bucciarelli-Ducci C., Bueno H., Caforio A.L., Crea F., Goudevenos J.A., Halvorsen S. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC) Eur. Heart J. 2018;39:119–177. - PubMed
-
- Collet J.-P., Thiele H., Barbato E., Barthélémy O., Bauersachs J., Bhatt D.L., Dendale P., Dorobantu M., Edvardsen T., Folliguet T. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC) Eur. Heart J. 2021;42:1289–1367. - PubMed
-
- Li Y.-H., Lee C.-H., Huang W.-C., Wang Y.-C., Su C.-H., Sung P.-H., Chien S.-C., Hwang J.-J. 2020 Focused Update of the 2012 Guidelines of the Taiwan Society of Cardiology for the Management of ST-Segment Elevation Myocardial Infarction. Acta Cardiol. Sin. 2020;36:285–307. doi: 10.6515/acs.202007_36(4).20200619a. - DOI - PMC - PubMed
-
- O’gara P.T., Kushner F.G., Ascheim D.D., Casey D.E., Jr., Chung M.K., De Lemos J.A., Ettinger S.M., Fang J.C., Fesmire F.M., Franklin B.A. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: Executive summary: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:529–555. doi: 10.1161/CIR.0b013e3182742c84. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
