

Epidemiological and Immunological Features of Obesity and SARS-CoV-2
- PMID: 34835041
- PMCID: PMC8624148
- DOI: 10.3390/v13112235
Epidemiological and Immunological Features of Obesity and SARS-CoV-2
Abstract
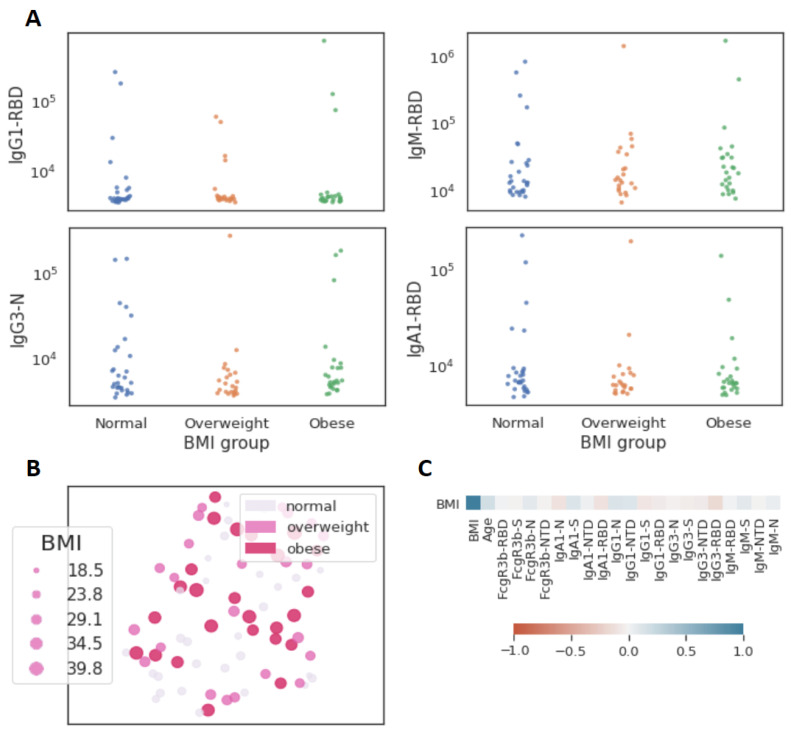
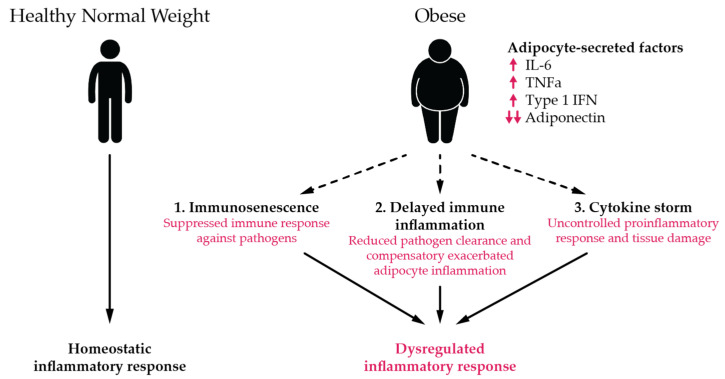
Obesity is a key correlate of severe SARS-CoV-2 outcomes while the role of obesity on risk of SARS-CoV-2 infection, symptom phenotype, and immune response remain poorly defined. We examined data from a prospective SARS-CoV-2 cohort study to address these questions. Serostatus, body mass index, demographics, comorbidities, and prior COVID-19 compatible symptoms were assessed at baseline and serostatus and symptoms monthly thereafter. SARS-CoV-2 immunoassays included an IgG ELISA targeting the spike RBD, multiarray Luminex targeting 20 viral antigens, pseudovirus neutralization, and T cell ELISPOT assays. Our results from a large prospective SARS-CoV-2 cohort study indicate symptom phenotype is strongly influenced by obesity among younger but not older age groups; we did not identify evidence to suggest obese individuals are at higher risk of SARS-CoV-2 infection; and remarkably homogenous immune activity across BMI categories suggests immune protection across these groups may be similar.
Keywords: COVID-19; SARS-CoV-2; body mass index; clinical features; epidemiology; immunity; obesity.
Conflict of interest statement
G.A. is a founder of Seromyx Systems Inc., a company developing platform technology that describes the antibody immune response. G.A.’s interests were reviewed and are managed by Massachusetts General Hospital in accordance with their conflict-of-interest policies. M.J.G. (Matthew J. Gluck), S.B., Y.H., J.R., E.P., B.M., A.S.M. and E.R.M. are employees of Space Exploration Technologies Corp. All other authors have declared that no conflict of interest exist.
Figures
Update of
-
Epidemiological and immunological features of obesity and SARS-CoV-2.medRxiv [Preprint]. 2020 Dec 11:2020.11.11.20229724. doi: 10.1101/2020.11.11.20229724. medRxiv. 2020. Update in: Viruses. 2021 Nov 06;13(11):2235. doi: 10.3390/v13112235. PMID: 33200139 Free PMC article. Updated. Preprint.
References
-
- WHO . Obesity and Overweight: Fact Sheet. WHO Media Centre; Geneva, Switzerland: 2020. [(accessed on 2 October 2020)]. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
-
- Tartof S.Y., Qian L., Hong M.V., Wei M.R., Nadjafi R.F., Fischer H., Li M.Z., Shaw D.S.F., Caparosa M.S.L., Nau C.L., et al. Obesity and Mortality Among Patients Diagnosed With COVID-19: Results From an Integrated Health Care Organization. Ann. Intern. Med. 2020;173:773–781. doi: 10.7326/M20-3742. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U19 AI135995/AI/NIAID NIH HHS/United States
- U19AI42790-01/NH/NIH HHS/United States
- R56 DA038366/DA/NIDA NIH HHS/United States
- R01 AI146785/AI/NIAID NIH HHS/United States
- U19 AI142790/AI/NIAID NIH HHS/United States
- 3R37AI080289-11S1/NH/NIH HHS/United States
- OPP1146996/GATES/Gates Foundation/United States
- INV-001650/NH/NIH HHS/United States
- R01AI146785/NH/NIH HHS/United States
- 1U01CA260476/NH/NIH HHS/United States
- 206250/Z/17/Z/WT_/Wellcome Trust/United Kingdom
- U01 CA260476/CA/NCI NIH HHS/United States
- R37 AI080289/AI/NIAID NIH HHS/United States
- U19AI135995-02/NH/NIH HHS/United States
- NNX16AO69A/NASA/NASA/United States
- CIVIC75N93019C00052/NH/NIH HHS/United States
- K24 DA037109/DA/NIDA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
