

Intestinal Dominance by Serratia marcescens and Serratia ureilytica among Neonates in the Setting of an Outbreak
- PMID: 34835397
- PMCID: PMC8624583
- DOI: 10.3390/microorganisms9112271
Intestinal Dominance by Serratia marcescens and Serratia ureilytica among Neonates in the Setting of an Outbreak
Abstract
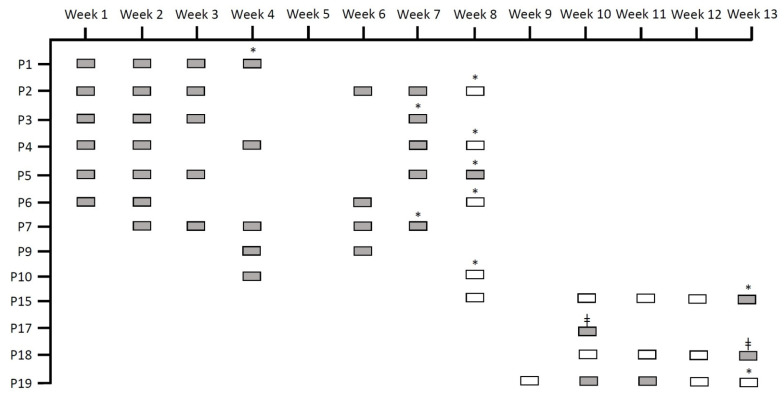
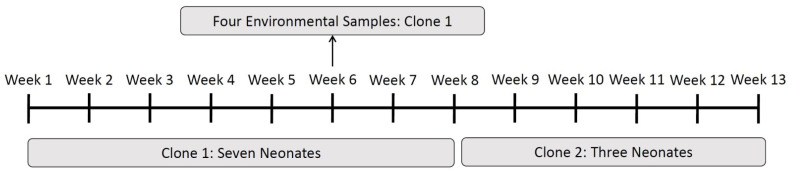
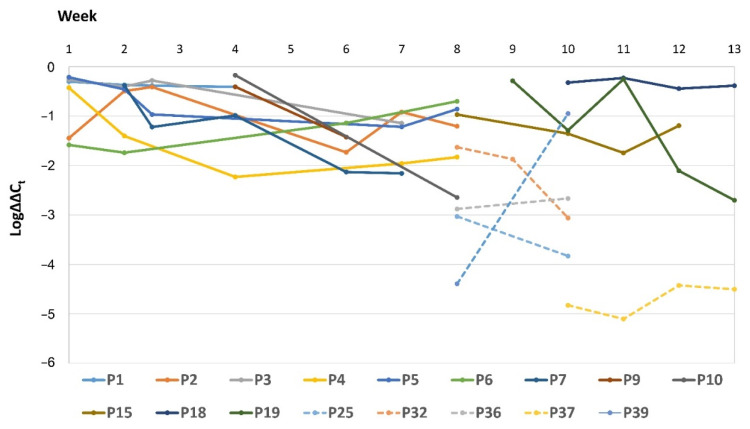
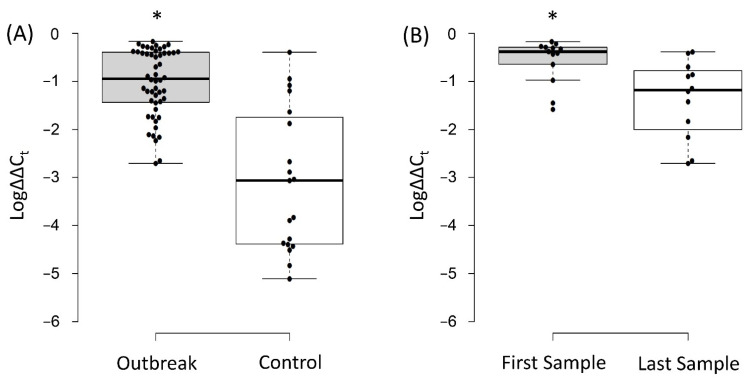
(1) Background: We determined the relevance of intestinal dominance by Serratia spp. during a neonatal outbreak over 13 weeks. (2) Methods: Rectal swabs (n = 110) were obtained from 42 neonates. Serratia spp. was cultured from swabs obtained from 13 neonates (Group 1), while the other 29 neonates were culture-negative (Group 2). Total DNA was extracted from rectal swabs, and quantitative PCRs (qPCRs) using Serratia- and 16SrRNA-gene-specific primers were performed. relative intestinal loads (RLs) were determined using ΔΔCt. Clonality was investigated by random amplified polymorphic DNA analysis and whole-genome sequencing. (3) Results: The outbreak was caused by Serratia marcescens during the first eight weeks and Serratia ureilytica during the remaining five weeks. Serratia spp. were detected by qPCR in all Group 1 neonates and eleven Group 2 neonates. RLs of Serratia spp. were higher in Group 1 as compared to Group 2 (6.31% vs. 0.09%, p < 0.05) and in the first swab compared to the last (26.9% vs. 4.37%, p < 0.05). Nine neonates had extraintestinal detection of Serratia spp.; eight of them were infected. RLs of the patients with extraintestinal spread were higher than the rest (2.79% vs. 0.29%, p < 0.05). (4) Conclusions: Intestinal dominance by Serratia spp. plays a role in outbreaks and extraintestinal spread.
Keywords: Serratia marcescens; Serratia ureilytica; intestinal dominance; neonatal ward; qPCR.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- The European Committee on Antimicrobial Susceptibility Testing (EUCAST) Expert Rules on Enterobacterales. Version 3.2. 2021. [(accessed on 19 October 2021)]. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Expert_Rule....
-
- Fisher M., Diago-Navarro E., Kaplun O., Sin E., Fries B.C. Serratia marcescens Strains Carrying blaKPC-2 and blaKPC-3 Carbapenemase Associated With Chronic Mechanical Ventilation. Open Forum Infect. Dis. 2018;5:S362. doi: 10.1093/ofid/ofy210.1029. - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
