

Glycogen Storage Disease Type Ia: Current Management Options, Burden and Unmet Needs
- PMID: 34836082
- PMCID: PMC8621617
- DOI: 10.3390/nu13113828
Glycogen Storage Disease Type Ia: Current Management Options, Burden and Unmet Needs
Abstract
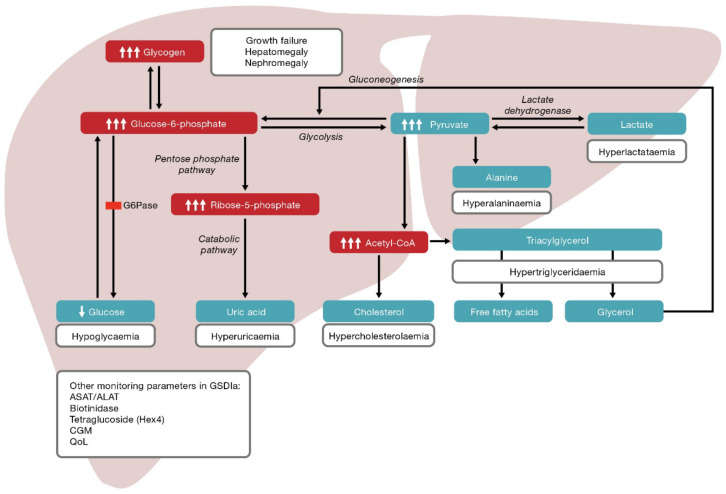
Glycogen storage disease type Ia (GSDIa) is caused by defective glucose-6-phosphatase, a key enzyme in carbohydrate metabolism. Affected individuals cannot release glucose during fasting and accumulate excess glycogen and fat in the liver and kidney, putting them at risk of severe hypoglycaemia and secondary metabolic perturbations. Good glycaemic/metabolic control through strict dietary treatment and regular doses of uncooked cornstarch (UCCS) is essential for preventing hypoglycaemia and long-term complications. Dietary treatment has improved the prognosis for patients with GSDIa; however, the disease itself, its management and monitoring have significant physical, psychological and psychosocial burden on individuals and parents/caregivers. Hypoglycaemia risk persists if a single dose of UCCS is delayed/missed or in cases of gastrointestinal intolerance. UCCS therapy is imprecise, does not treat the cause of disease, may trigger secondary metabolic manifestations and may not prevent long-term complications. We review the importance of and challenges associated with achieving good glycaemic/metabolic control in individuals with GSDIa and how this should be balanced with age-specific psychosocial development towards independence, management of anxiety and preservation of quality of life (QoL). The unmet need for treatment strategies that address the cause of disease, restore glucose homeostasis, reduce the risk of hypoglycaemia/secondary metabolic perturbations and improve QoL is also discussed.
Keywords: burden of disease; dietary treatment; glycogen storage disease type Ia; long-term complications; quality of life; uncooked cornstarch; unmet need.
Conflict of interest statement
T.G.J.D.: Adviser for Moderna Therapeutics and Ultragenyx Pharmaceutical Inc. and principal investigator for Ultragenyx Pharmaceutical Inc, and Vitaflo International Ltd.; D.F.R.-B.: Adviser for BioMarin Pharmaceutical Inc., adviser and principal investigator for Ultragenyx Pharmaceutical Inc; A.A.: Clinical investigator for clinical trials sponsored by Applied Therapeutics, Moderna Inc. and Ultragenyx Pharmaceutical Inc.; F.d.B.: No conflicts of interest to declare; M.L.C.: No conflicts of interest to declare; S.C.G.: Honoraria for lectures and/or advisory services from MetaX, Orphan Europe, Sobi and Vitaflo; P.L.: No conflicts of interest to declare; N.L.M.: No conflicts of interest to declare; C.F.M.d.S.: No conflicts of interest to declare; R.R.-W.: Clinical Investigator for Ultragenyx Pharmaceutical Inc.; A.R.: Grant recipient (research) Nutricia Metabolics and (travel) Ultragenyx Pharmaceutical Inc and Vitaflo Italia; H.S.: Consultant and member of speaker bureau for BioMarin Pharmaceutical Inc. and consultant for Moderna Therapeutics: R.N.G.: Employee and shareholder of Ultragenyx Pharmaceutical Inc.; V.V.: Employee and shareholder of Ultragenyx Pharmaceutical Inc.; J.M.: Clinical investigator for BioMarin Pharmaceutical Inc., Regenxbio, Rezolute Inc., Sanofi Genzyme, Takeda and Ultragenyx Pharmaceutical Inc. and consultant for BioMarin Pharmaceutical Inc., Sanofi Genzyme, Takeda and Ultragenyx Pharmaceutical Inc. The authors confirm their independence from the sponsors; the content of the article has not been influenced by the sponsors.
Figures
References
-
- De León D.D., Stanley C.A., Sperling M.A. Hypoglycemia in neonates and infants. In: Sperling M.A., editor. Pediatric Endocrinology. 3rd ed. W.B. Saunders; Philadelphia, PA, USA: 2008. pp. 165–197.
-
- Burr I.M., O’Neill J.A., Karzon D.T., Howard L.J., Greene H.L. Comparison of the effects of total parenteral nutrition, continuous intragastric feeding, and portacaval shunt on a patient with type I glycogen storage disease. J. Pediatr. 1974;85:792–795. doi: 10.1016/S0022-3476(74)80342-2. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
