

Scientific and clinical developments in Merkel cell carcinoma: A polyomavirus-driven, often-lethal skin cancer
- PMID: 34836718
- PMCID: PMC8810602
- DOI: 10.1016/j.jdermsci.2021.10.004
Scientific and clinical developments in Merkel cell carcinoma: A polyomavirus-driven, often-lethal skin cancer
Abstract
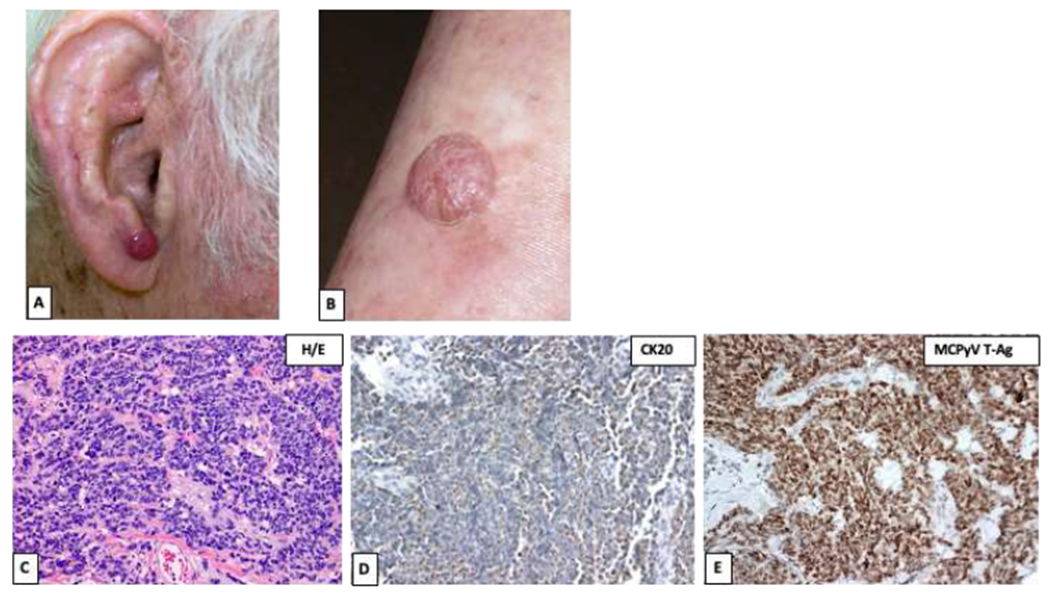
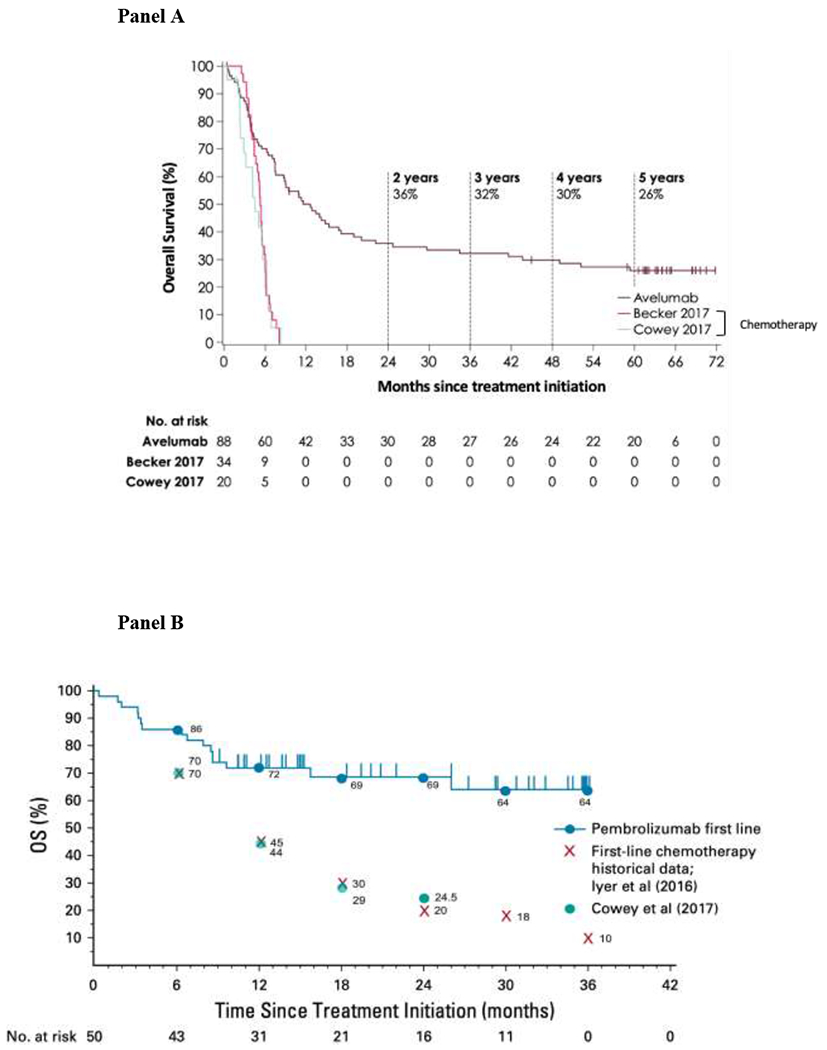
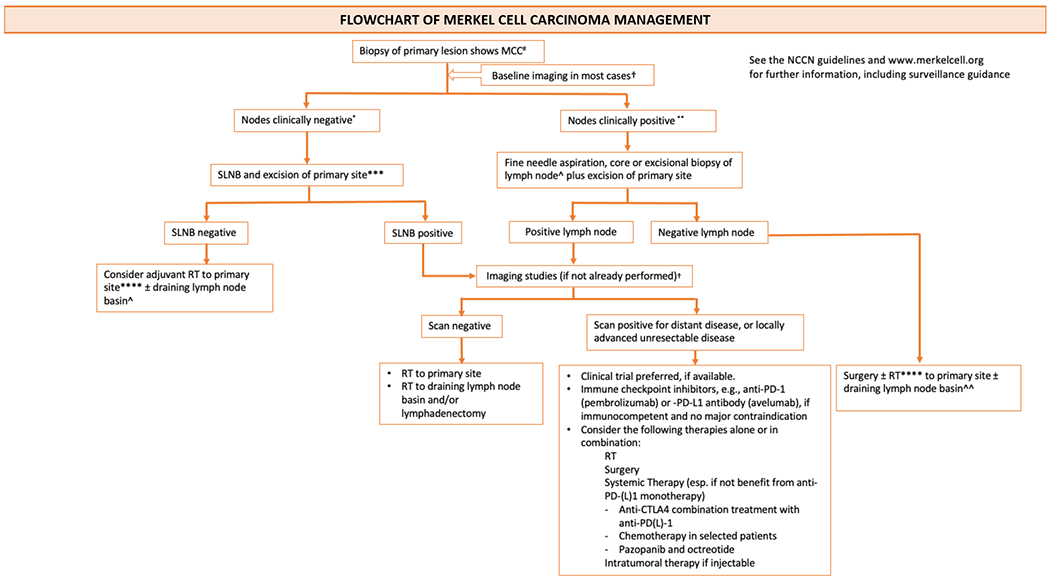
Merkel cell carcinoma (MCC) is a primary neuroendocrine skin cancer that recurs in ~40% of cases. Merkel cell polyomavirus (MCPyV) and ultraviolet (UV)-induced mutations are two major causative factors of MCC. Virus-positive MCCs express polyomavirus oncoproteins that are highly immunogenic yet are required for ongoing tumor growth. Virus-negative MCCs have a high burden of UV-DNA mutations that encode tumor-specific UV-neoantigens. Thus, both UV- and virus-induced MCCs are highly immunogenic, enabling diverse T-cell targeted therapies. Optimal MCC management is challenging given its rarity, aggressive nature, rapidly evolving care guidelines, and fundamental differences in management compared to other skin cancers. MCC is often managed aggressively with extensive surgery, radiotherapy or systemic therapy, frequently leading to toxicities that might have been avoidable while still achieving optimal disease control. Thus, multi-disciplinary care is crucial for providing patients with the best possible outcomes. The outlook for many patients with advanced MCC has progressed remarkably over the past decade due to PD-1 pathway blocking agents that provide durable benefit for a substantial subset of MCC patients. The management of early-stage MCC has also improved due to better approaches to integrate surgery and radiotherapy. Prognostic accuracy and ongoing surveillance have advanced due to stage-specific recurrence data and sophisticated "liquid biopsies" that allow early detection of disease recurrence. Here we summarize both recent striking progress and pressing challenges such as PD-(L)1-refractory MCC, and management of MCC patients with immune dysfunction. We also highlight diverse resources to allow providers to take advantage of recent progress in this fast-moving field.
Keywords: Cutaneous neuroendocrine carcinoma; Immunotherapy; Merkel cell carcinoma; Merkel cell polyomavirus; Multidisciplinary care.
Copyright © 2021 Japanese Society for Investigative Dermatology. Published by Elsevier B.V. All rights reserved.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
