

Assessing the prognostic utility of smoldering multiple myeloma risk stratification scores applied serially post diagnosis
- PMID: 34836942
- PMCID: PMC8626440
- DOI: 10.1038/s41408-021-00569-2
Assessing the prognostic utility of smoldering multiple myeloma risk stratification scores applied serially post diagnosis
Abstract
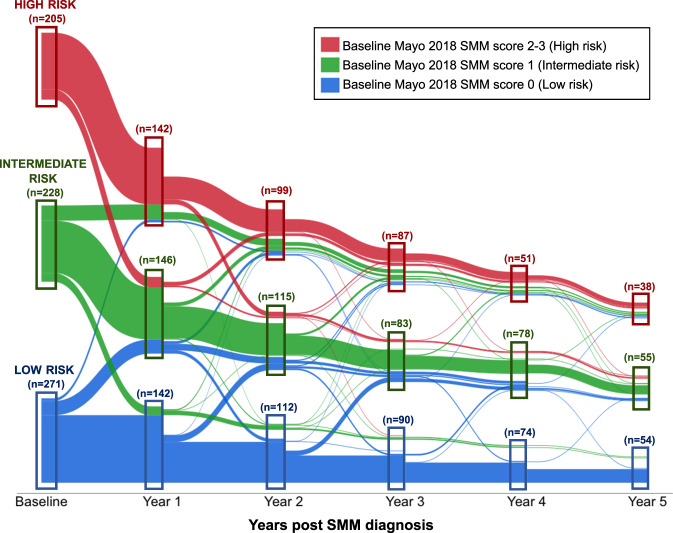
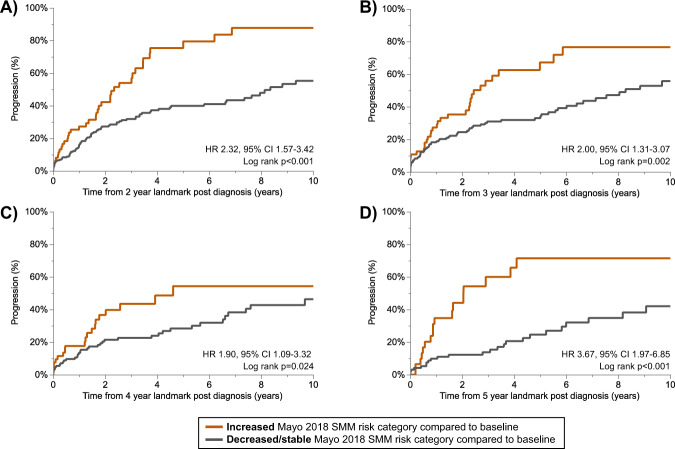
The Mayo-2018 smoldering multiple myeloma (SMM) risk score is used routinely in the clinical setting but has only been validated at diagnosis. In SMM patients, the progression risk decreases over time. However, the utility of applying risk stratification models after diagnosis is unknown. We retrospectively studied 704 SMM patients and applied the Mayo 2018 and IMWG-2020 risk stratification models at annual landmark timepoints up to 5 years post diagnosis. The Mayo-2018 and IMWG-2020 models reliably stratified patients based on progression risk when applied post diagnosis. The respective 2-year progression risk in Mayo-2018 high risk patients versus IMWG-2020 intermediate-high risk patients was 51% versus 62% at the 1-year landmark and 47% versus 45% at the 4-year landmark. We showed that patients categorized at Mayo-2018 high-risk at follow-up had a similar risk of progression if the baseline risk assessment was low-intermediate versus high-risk (HR 1.04, 95% CI 0.46-2.36, p = 0.931 at 5-year landmark). Patients migrating to a higher risk category during follow up had a higher progression risk compared to patients with stable/decreased risk categorization. Our findings support the use of these risk scores post-diagnosis and suggest that patients evolving to a high-risk category may benefit from early intervention therapeutic approaches.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Mateos MV, Hernández MT, Giraldo P, de la Rubia J, de Arriba F, Corral LL, et al. Lenalidomide plus dexamethasone versus observation in patients with high-risk smouldering multiple myeloma (QuiRedex): long-term follow-up of a randomised, controlled, phase 3 trial. Lancet Oncol. 2016;17:1127–36.. doi: 10.1016/S1470-2045(16)30124-3. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
