

Regional variations in hepatocellular carcinoma incidence, routes to diagnosis, treatment and survival in England
- PMID: 34837073
- PMCID: PMC8888669
- DOI: 10.1038/s41416-021-01509-4
Regional variations in hepatocellular carcinoma incidence, routes to diagnosis, treatment and survival in England
Abstract
Background: Hepatocellular carcinoma (HCC) incidence, management and survival across England were examined to determine if geographical inequalities exist.
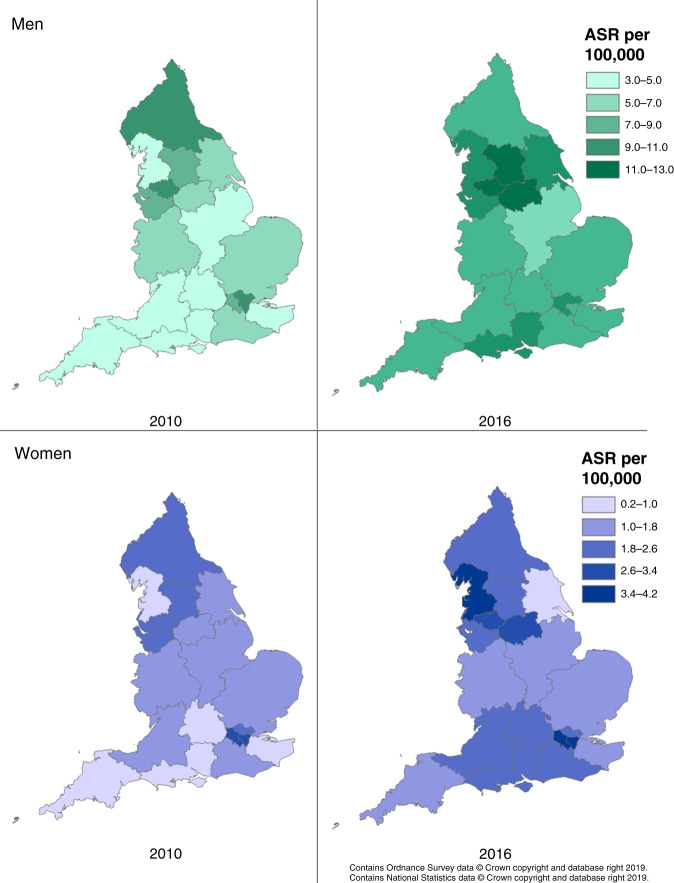
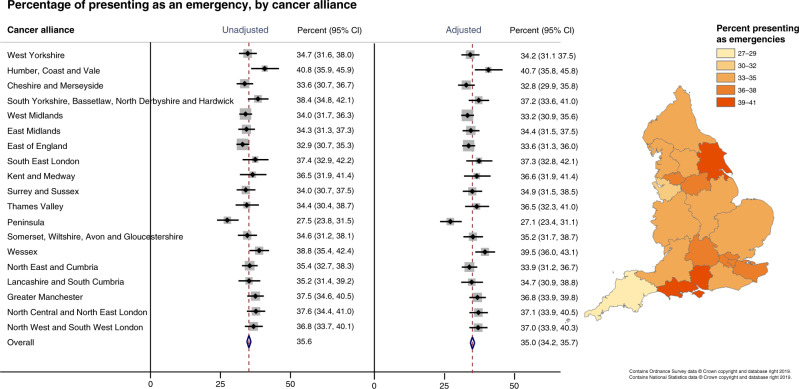
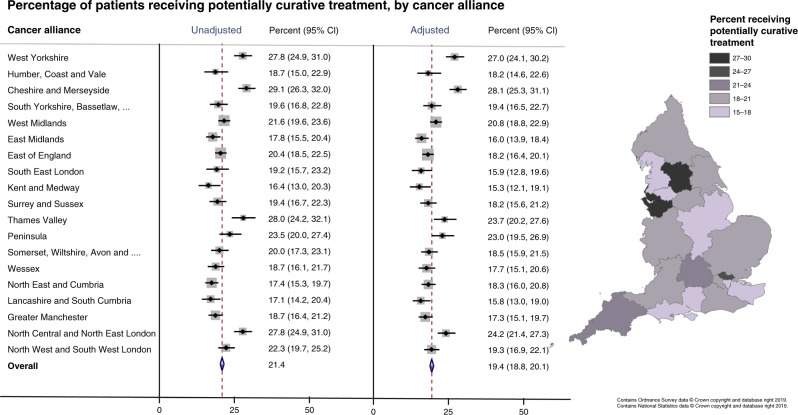
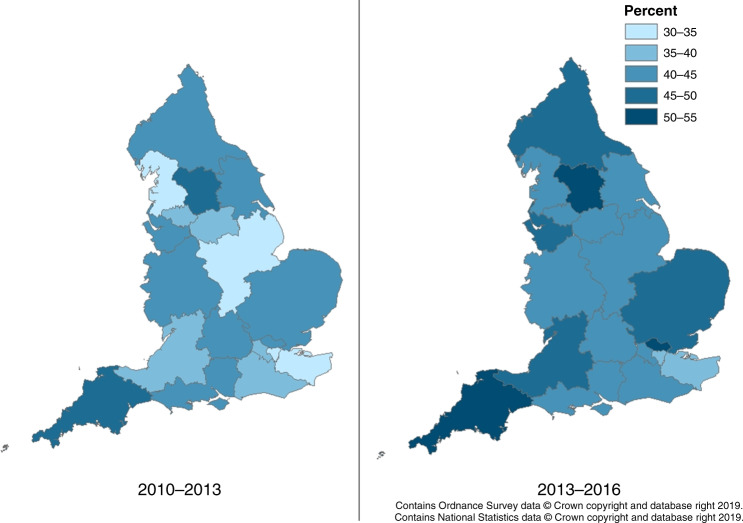
Method: 15,468 HCC cases diagnosed 2010-2016 were included. Age-standardised incidence rates, net survival and proportions receiving potentially curative treatment and presenting through each route to diagnosis adjusted for age at diagnosis, sex and area-based deprivation quintile, were calculated overall and by Cancer Alliance.
Results: HCC incidence rates increased in men from 6.2 per 100,000 in 2010 to 8.8 in 2016, and in women from 1.5 to 2.2. The highest incidence rates, found in parts of the North of England and London, were nearly double the lowest. The adjusted proportion presenting as an emergency ranged 27-41% across Cancer Alliances. Odds increased with increasing deprivation quintile and age. Only one in five patients received potentially curative treatment (range 15-28%) and odds decreased with increasing deprivation and age. One-year survival in 2013-2016 ranged 38-53%.
Conclusion: This population-based, nationwide analysis demonstrates clear differences in HCC incidence, management and survival across England. It highlights socioeconomic-associated variation and the need for improvement in early diagnosis and curative treatment of HCC. This research should assist policymakers, service providers and clinicians to identify regions where additional training, services and resources would be best directed.
© 2021. The Author(s).
Conflict of interest statement
All of the authors completed the ICMJE uniform disclosure form; Professor Alexander, Dr. Tataru, Ms. Paley, Dr. Marshall and Dr. Driver have nothing to disclose. During the conduct of the study, Dr. Burton reports grants from BTG International Ltd and Dr. Balachandrakumar, Dr. Cross and Professor Palmer report grants from Sirtex, Bristol-Myers-Squibb and Bayer. Dr Cross reports personal fees from Bayer. Outside the submitted work, Dr. Cross reports personal fees from Eisai pharmaceuticals, Bayer, AstraZeneca and Roche and Professor Palmer reports grants and personal fees from Bristol-Myers-Squibb, AstraZeneca, MSD and Nucana Inc, and personal fees from Eisai, Bayer, and Roche. Dr. Rowe reports personal fees from Roche, non-financial support from Abbvie, outside the submitted work.
Figures
References
-
- Liu Z, Jiang Y, Yuan H, Fang Q, Cai N, Suo C, et al. The trends in incidence of primary liver cancer caused by specific etiologies: results from the Global Burden of Disease Study 2016 and implications for liver cancer prevention. J Hepatol. 2019;70:674–83. doi: 10.1016/j.jhep.2018.12.001. - DOI - PubMed
-
- The 2nd Atlas of variation in risk factors and healthcare for liver disease in England. (Public Health England, Wellington House, London SE1 8UG, 2017).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
