

Which is the best transcranial direct current stimulation protocol for migraine prevention? A systematic review and critical appraisal of randomized controlled trials
- PMID: 34837963
- PMCID: PMC8903540
- DOI: 10.1186/s10194-021-01361-0
Which is the best transcranial direct current stimulation protocol for migraine prevention? A systematic review and critical appraisal of randomized controlled trials
Abstract
Background: Transcranial direct current stimulation (tDCS) could counteract the pathophysiological triggers of migraine attacks by modulating cortical excitability. Several pilot randomized controlled trials (RCTs) assessed the efficacy of tDCS for migraine prevention. We reviewed and summarized the state of the art of tDCS protocols for migraine prevention, discussing study results according to the stimulations parameters and patients' populations.
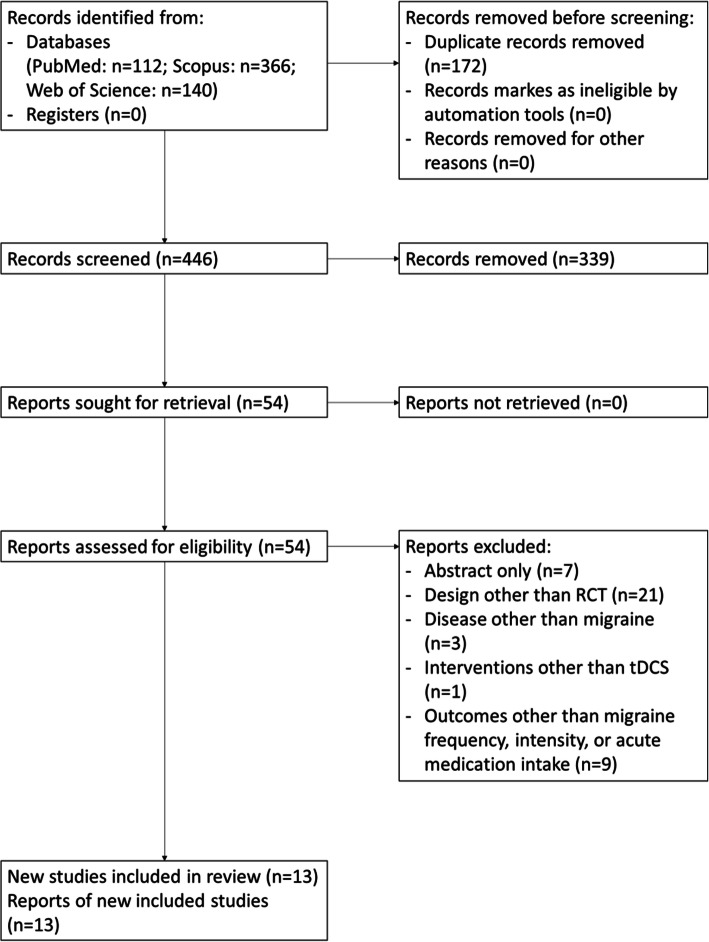
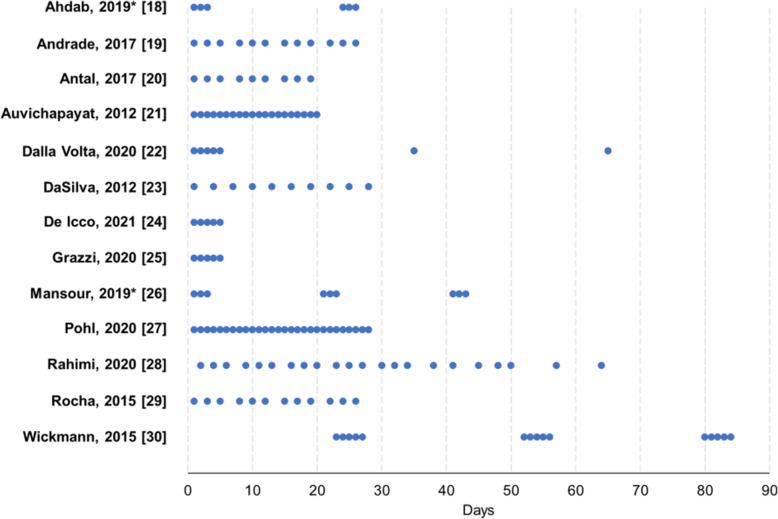
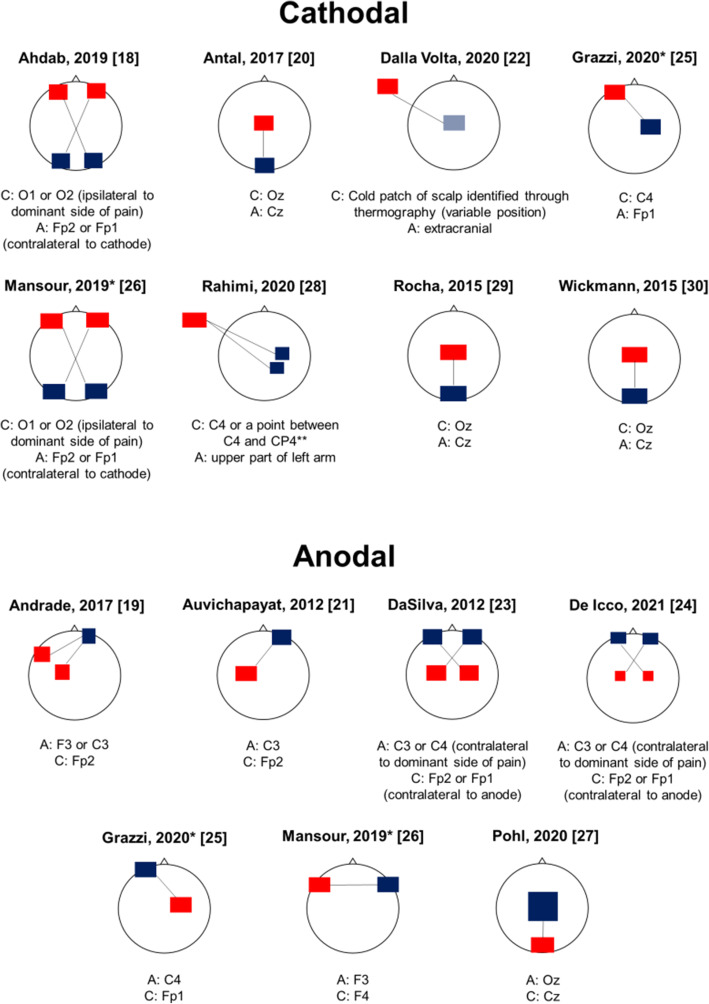
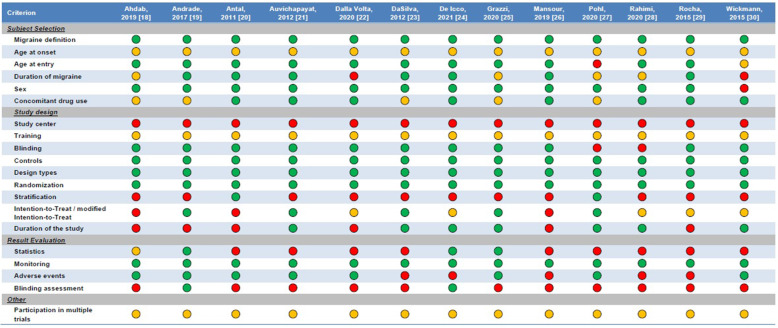
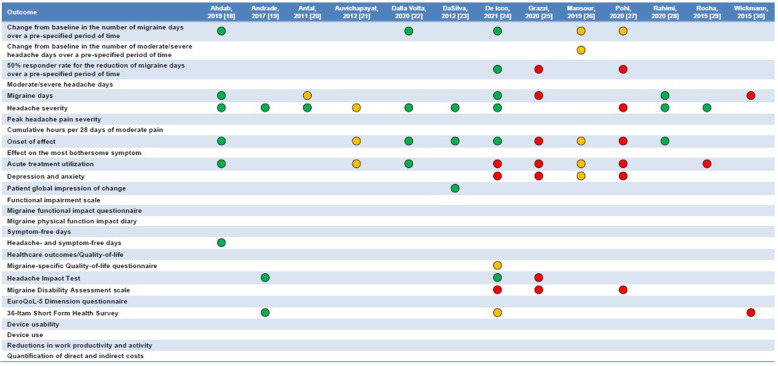
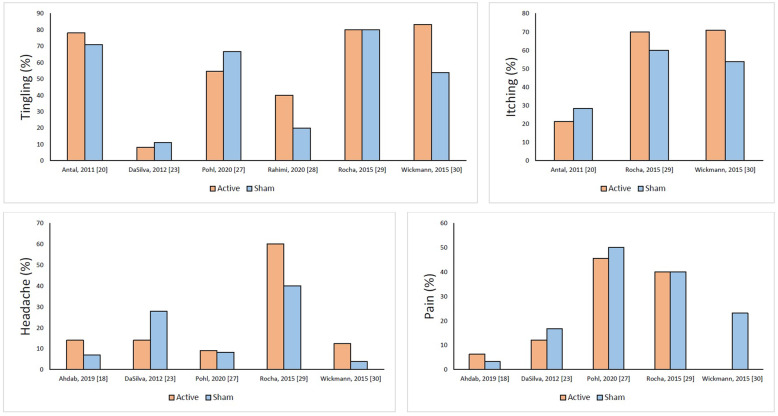
Main body: We combined the keywords 'migraine', 'headache', 'transcranial direct current stimulation', and 'tDCS' and searched Pubmed, Scopus, and Web of Science, from the beginning of indexing to June 22, 2021. We only included RCTs comparing the efficacy of active tDCS with sham tDCS to decrease migraine frequency, intensity, and/or acute drug utilization. The risk of bias of each RCT was assessed by using the RoB-2 tool (Cochrane Collaboration). Thirteen RCTs (from 2011 to 2021) were included in the review. The included patients ranged from 13 to 135. RCTs included patients with any migraine (n=3), chronic migraine (n=6), episodic migraine (n=3) or menstrual migraine (n=1). Six RCTs used cathodal and five anodal tDCS, while two RCTs compared the efficacy of both cathodal and anodal tDCS with that of sham. In most of the cathodal stimulation trials, the target areas were the occipital regions, with reference on central or supraorbital areas. In anodal RCTs, the anode was usually placed above the motor cortical areas and the cathode on supraorbital areas. All RCTs adopted repeated sessions (from 5 to 28) at variable intervals, while the follow-up length spanned from 1 day up to 12 months. Efficacy results were variable but overall positive. According to the RoB-2 tool, only four of the 13 RCTs had a low risk of bias, while the others presented some concerns.
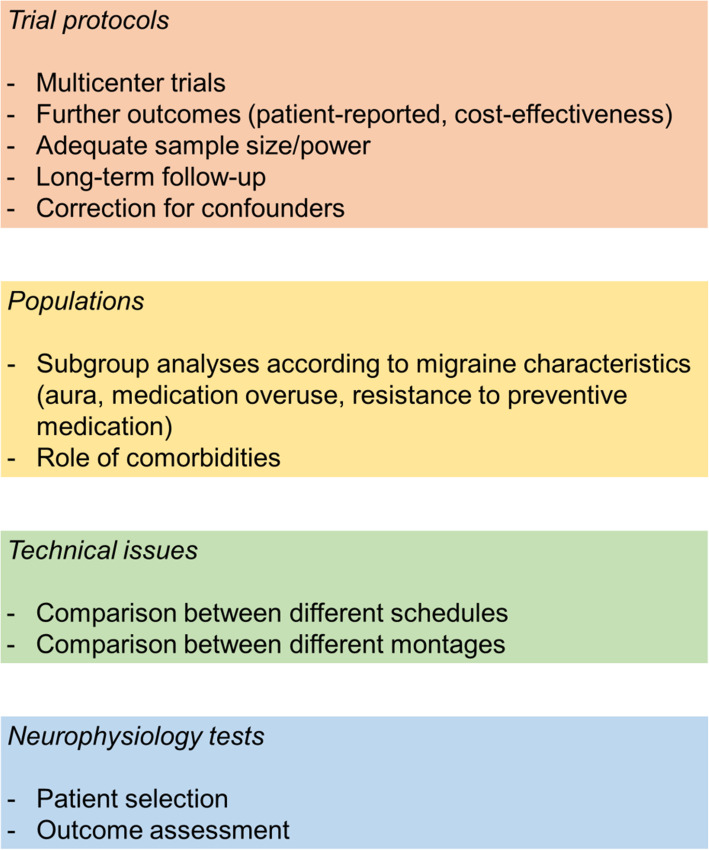
Conclusions: Both anodal and cathodal tDCS are promising for migraine prevention. However, there is a need for larger and rigorous RCTs and standardized procedures. Additionally, the potential benefits and targeted neurostimulation protocols should be assessed for specific subgroups of patients.
Keywords: Transcranial direct current stimulation; migraine; migraine prevention; non-pharmacological treatment.
© 2021. The Author(s).
Conflict of interest statement
RO reports personal fees from Novartis, Teva, and Eli Lilly, and had non-financial relationships with Allergan/AbbVie, Novartis and Teva. SS reports personal fees and nonfinancial support from Allergan, Abbott, Eli Lilly, Lundbeck, Novartis, and Teva; personal fees from Medscape; and other from Bayer, Pfizer, Medtronic, Starmed, Bristol-Myers Squibb, and Daiichi Sankyo. The remaining Authors declare no competing interests.
Figures
References
-
- Burch R. Preventive Migraine Treatment. Continuum (Minneap Minn) 2021;27(3):613–632. - PubMed
-
- Sacco S, Braschinsky M, Ducros A, Lampl C, Little P, van den Brink AM, et al. European headache federation consensus on the definition of resistant and refractory migraine : Developed with the endorsement of the European Migraine & Headache Alliance (EMHA) J Headache Pain. 2020;21(1):76. - PMC - PubMed
-
- Charles A. The pathophysiology of migraine: implications for clinical management. Lancet Neurol. 2018;17(2):174–182. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
