

Non-invasive detection of a femoral-to-radial arterial pressure gradient in intensive care patients with vasoactive agents
- PMID: 34838150
- PMCID: PMC8627053
- DOI: 10.1186/s40560-021-00585-1
Non-invasive detection of a femoral-to-radial arterial pressure gradient in intensive care patients with vasoactive agents
Abstract
Background: In patient requiring vasopressors, the radial artery pressure may underestimate the true central aortic pressure leading to unnecessary interventions. When using a femoral and a radial arterial line, this femoral-to-radial arterial pressure gradient (FR-APG) can be detected. Our main objective was to assess the accuracy of non-invasive blood pressure (NIBP) measures; specifically, measuring the gradient between the NIBP obtained at the brachial artery and the radial artery pressure and calculating the non-invasive brachial-to-radial arterial pressure gradient (NIBR-APG) to detect an FR-APG. The secondary objective was to assess the prevalence of the FR-APG in a targeted sample of critically ill patients.
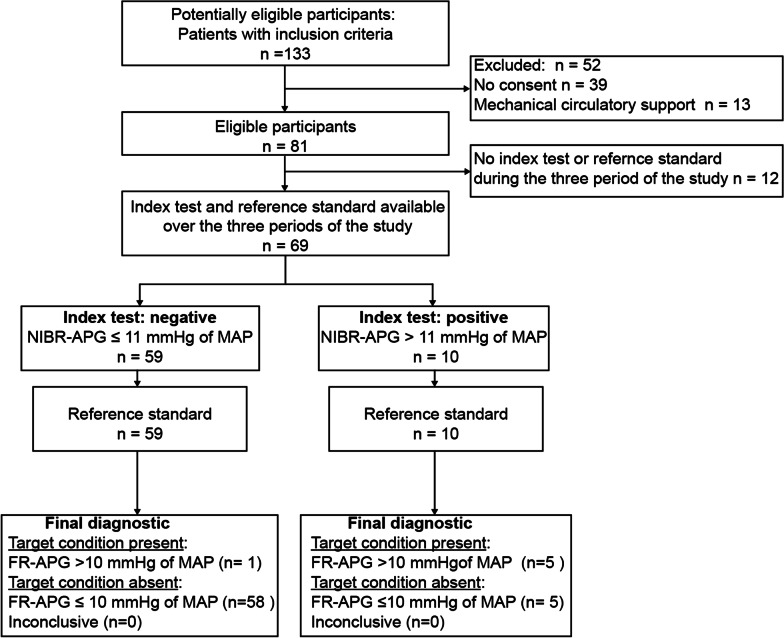
Methods: Adult patients in an intensive care unit requiring vasopressors and instrumented with a femoral and a radial artery line were selected. We recorded invasive radial and femoral arterial pressure, and brachial NIBP. Measurements were repeated each hour for 2 h. A significant FR-APG (our reference standard) was defined by either a mean arterial pressure (MAP) difference of more than 10 mmHg or a systolic arterial pressure (SAP) difference of more than 25 mmHg. The diagnostic accuracy of the NIBR-APG (our index test) to detect a significant FR-APG was estimated and the prevalence of an FR-APG was measured and correlated with the NIBR-APG.
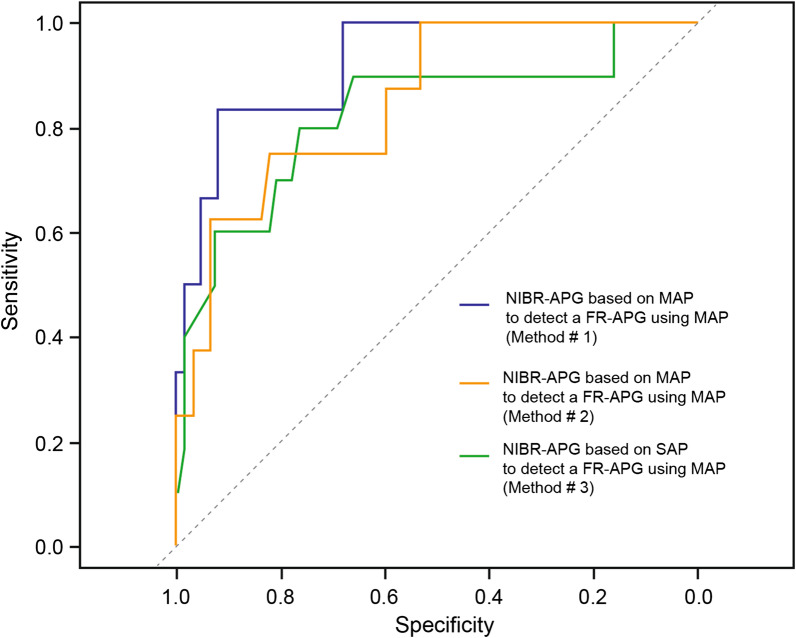
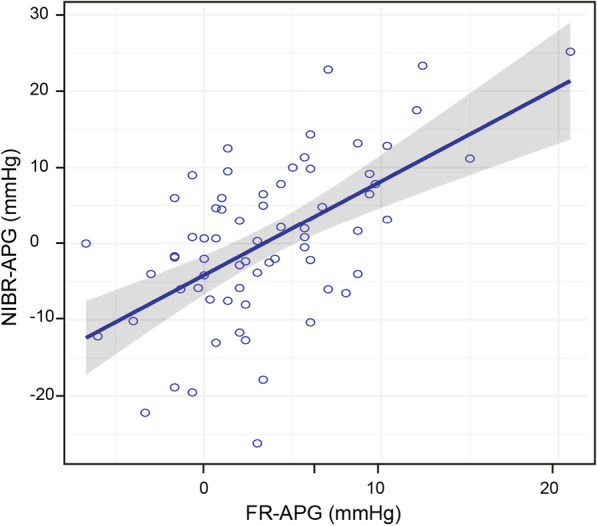
Results: Eighty-one patients aged 68 [IQR 58-75] years and an SAPS2 score of 35 (SD 7) were included from which 228 measurements were obtained. A significant FR-APG occurred in 15 patients with a prevalence of 18.5% [95%CI 10.8-28.7%]. Diabetes was significantly associated with a significant FR-APG. The use of a 11 mmHg difference in MAP between the NIBP at the brachial artery and the MAP of the radial artery led to a specificity of 92% [67; 100], a sensitivity of 100% [95%CI 83; 100] and an AUC ROC of 0.93 [95%CI 0.81-0.99] to detect a significant FR-APG. SAP and MAP FR-APG correlated with SAP (r2 = 0.36; p < 0.001) and MAP (r2 = 0.34; p < 0.001) NIBR-APG.
Conclusion: NIBR-APG assessment can be used to detect a significant FR-APG which occur in one in every five critically ill patients requiring vasoactive agents.
Keywords: Aorto-radial gradient; Diagnostic study; Femoro-radial gradient; Vasoplegia.
© 2021. The Author(s).
Conflict of interest statement
Dr. Denault is speaker and consultant for CAE Healthcare, and speaker for Edwards and Masimo. He received a research grant from Edwards (2019).
Figures
References
-
- Manecke GR, Jr, Parimucha M, Stratmann G, Wilson WC, Roth DM, Auger WR, Kerr KM, Jamieson SW, Kapelanski DP, Mitchell MM. Deep hypothermic circulatory arrest and the femoral-to-radial arterial pressure gradient. J Cardiothorac Vasc Anesth. 2004;18(2):175–179. doi: 10.1053/j.jvca.2004.01.023. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
