

How many is too many? Polyposis syndromes and what to do next
- PMID: 34839308
- PMCID: PMC8648991
- DOI: 10.1097/MOG.0000000000000796
How many is too many? Polyposis syndromes and what to do next
Abstract
Purpose of review: The goal of this review is to help providers recognize, diagnose and manage gastrointestinal (GI) polyposis syndromes.
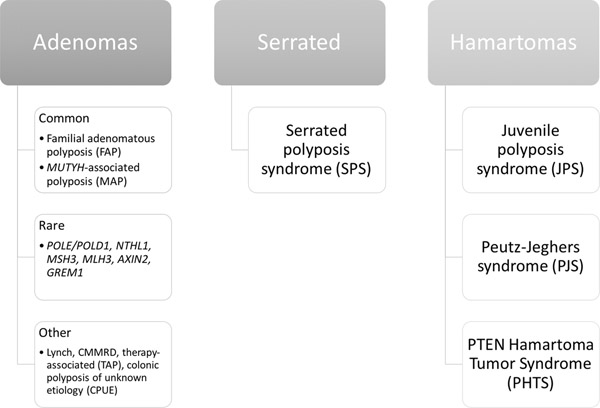
Recent findings: Intestinal polyps include a number of histological sub-types such as adenomas, serrated, hamartomas among others. Over a quarter of individuals undergoing screening colonoscopy are expected to have colonic adenomas. Although it is not uncommon for adults to have a few GI polyps in their lifetime, some individuals are found to have multiple polyps of varying histology throughout the GI tract. In these individuals, depending on polyp histology, number, location and size as well as extra-intestinal features and/or family history, a polyposis syndrome should be considered with appropriate testing and management.
Summary: Diagnosis and management of polyposis syndromes has evolved with advent of multigene panel testing and new data on optimal surveillance strategies. Evidence-based recommendations and current practice guidelines for polyposis syndromes are reviewed here. Areas of uncertainty and future research are also highlighted.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
3.
Figures
References
-
-
National Comprehensive Cancer Network, Inc. 2021. Genetic/Familial High Risk Assessment: Colorectal v.1.2021 Available at https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1436.
** NCCN summarizes their management recommendations for individuals with polyposis, which differs by mutated gene. NCCN guidelines are updated on a regular basis when new evidence becomes available.
-
-
-
Heald B, Hampel H, Church J, Dudley B, Hall MJ, Mork ME, et al. Collaborative Group of the Americas on Inherited Gastrointestinal Cancer Position statement on multigene panel testing for patients with colorectal cancer and/or polyposis. Fam Cancer. 2020. July;19(3):223–39.
** Collaborative Group of the Americas on Inherited Gastrointestinal Cancers published their position statement on genetic testing in polyposis, who recommend multi-gene panel testing given the number of polyposis syndromes (which can have overlapping features), and improvements in sequencing technology. They recommend that individuals with 10+ adenomas or 3+ hamartomatous polyps should undergo multi-gene panel testing. This statement also includes review of the minimum gene set to be used when testing individuals for a polyposis syndrome.
-
-
- Serrated polyposis syndrome [Internet]. InSiGHT. [cited 2021 Aug 18]. Available from: https://www.insight-group.org/syndromes/serrated-polyposis-syndrome/
-
-
Stanich PP, Pearlman R, Hinton A, Gutierrez S, LaDuca H, Hampel H, et al. Prevalence of Germline Mutations in Polyposis and Colorectal Cancer–Associated Genes in Patients With Multiple Colorectal Polyps. Clin Gastroenterol Hepatol. 2019. September 1;17(10):2008–2015.e3.
** Stanich et al summarizes genetic findings of 3789 patients and found that the chance to find a P/LP variant increases with age in adenomatous polyposis. With the exception of APC and MUTYH, pathogenic/likely pathogenic variants in adenomatous polyposis genes are rare. This study also showed that adenoma count is also associated with finding a pathogenic or likely pathogenic variant.
-
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
