

CMR-derived myocardial strain analysis differentiates ischemic and dilated cardiomyopathy-a propensity score-matched study
- PMID: 34839396
- PMCID: PMC11130031
- DOI: 10.1007/s10554-021-02469-9
CMR-derived myocardial strain analysis differentiates ischemic and dilated cardiomyopathy-a propensity score-matched study
Abstract
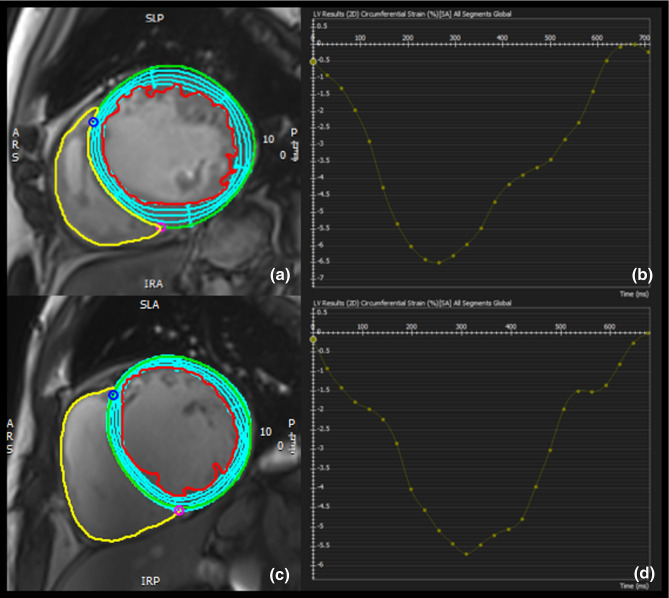
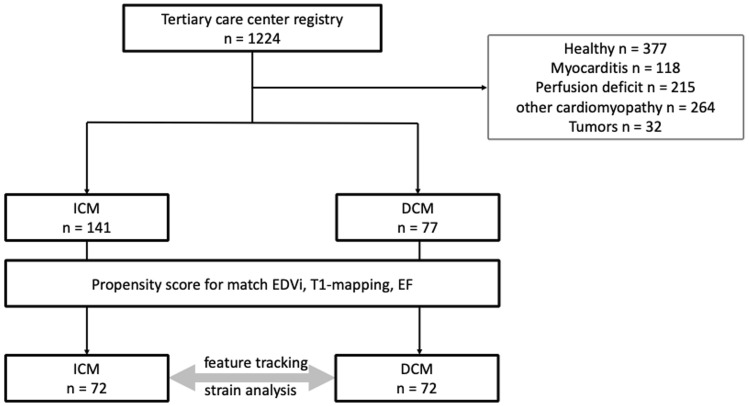
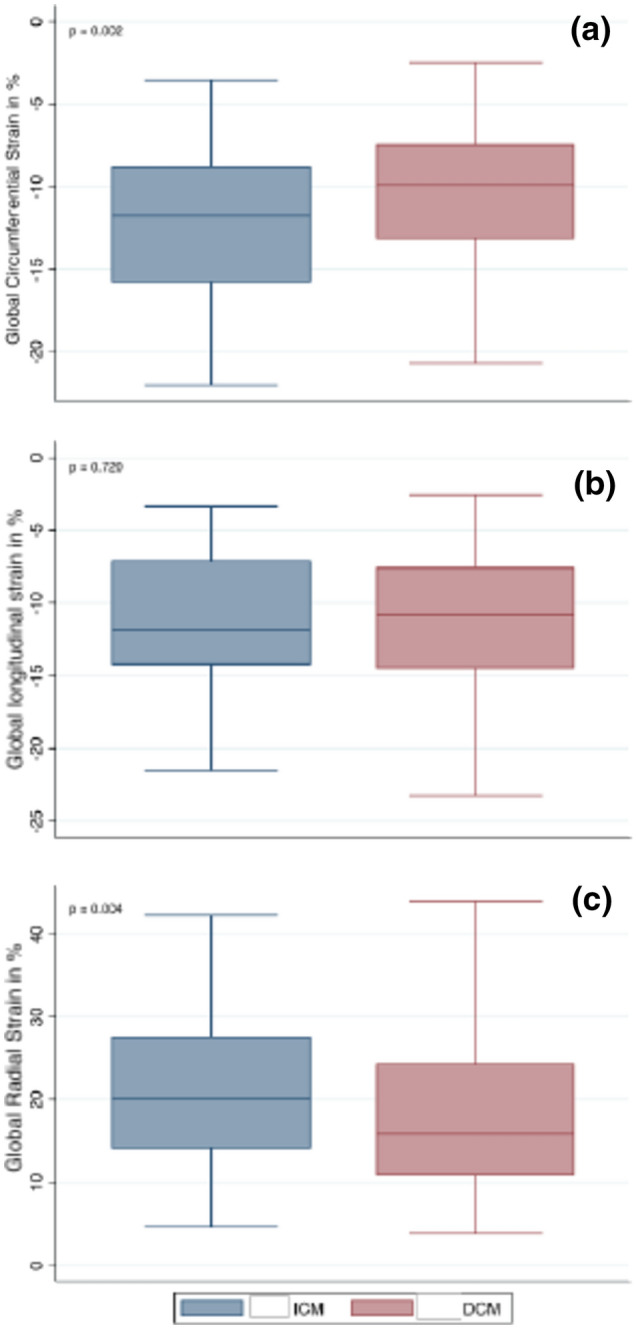
Left ventricular (LV) longitudinal, circumferential, and radial motion can be measured using feature tracking of cardiac magnetic resonance (CMR) images. The aim of our study was to detect differences in LV mechanics between patients with dilated cardiomyopathy (DCM) and ischemic cardiomyopathy (ICM) who were matched using a propensity score-based model. Between April 2017 and October 2019, 1224 patients were included in our CMR registry, among them 141 with ICM and 77 with DCM. Propensity score matching was used to pair patients based on their indexed end-diastolic volume (EDVi), ejection fraction (EF), and septal T1 relaxation time (psmatch2 module L Feature tracking provided six parameters for global longitudinal, circumferential, and radial strain with corresponding strain rates in each group. Strain parameters were compared between matched pairs of ICM and DCM patients using paired t tests. Propensity score matching yielded 72 patients in each group (DCM mean age 58.6 ± 11.6 years, 15 females; ICM mean age 62.6 ± 13.2 years, 11 females, p = 0.084 and 0.44 respectively; LV-EF 32.2 ± 13.5% vs. 33.8 ± 12.1%, p = 0.356; EDVi 127.2 ± 30.7 ml/m2 vs. 121.1 ± 41.8 ml/m2, p = 0.251; native T1 values 1165 ± 58 ms vs. 1167 ± 70 ms, p = 0.862). There was no difference in global longitudinal strain between DCM and ICM patients (- 10.9 ± 5.5% vs. - 11.2 ± 4.7%, p = 0.72), whereas in DCM patients there was a significant reduction in global circumferential strain (- 10.0 ± 4.5% vs. - 12.2 ± 4.7%, p = 0.002) and radial strain (17.1 ± 8.51 vs. 21.2 ± 9.7%, p = 0.039). Our data suggest that ICM and DCM patients have inherently different myocardial mechanics, even if phenotypes are similar. Our data show that GCS is significantly more impaired in DCM patients. This feature may help in more thoroughly characterizing cardiomyopathy patients.
Keywords: CMR; Feature tracking; Heart failure; Strain.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Reimer KA, Jennings RB. The "wavefront phenomenon" of myocardial ischemic cell death. II. Transmural progression of necrosis within the framework of ischemic bed size (myocardium at risk) and collateral flow. Lab Invest. 1979;40:633–644. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
