

Review
doi: 10.1016/j.bjae.2021.07.007.
Epub 2021 Sep 21.
Clinical anatomy of the nerve supply to the upper limb
Affiliations
- PMID: 34840818
- PMCID: PMC8606604
- DOI: 10.1016/j.bjae.2021.07.007
Item in Clipboard
Review
Clinical anatomy of the nerve supply to the upper limb
BJA Educ.
2021 Dec.
No abstract available
Keywords: anaesthesia; anaesthesia, conduction; anatomy; brachial plexus.
Figures

Simplified brachial plexus anatomy demonstrating the different points at which it divides with the anatomical locations of plexus blocks and subsequent cutaneous sensory coverage. Inset image demonstrates the ‘hourglass’ shape of the plexus. Note that the nerve roots in the cervical region (C5–8) emerge above the corresponding vertebra, whilst the T1 nerve root appears below. A, axillary nerve; M, median nerve; Mc, musculocutaneous nerve; R, radial nerve; U, ulnar nerve.

Computer-generated image from cadaveric specimen demonstrating the dissected brachial plexus, including its relationship to the major arteries.

Cutaneous sensory distribution of the arm and forearm Original image courtesy of Professor Alice Roberts. inf., inferior; lat., lateral; n., nerve.

Ulnar claw hand deformity. Reprinted from Hussain and Winterton, with permission.
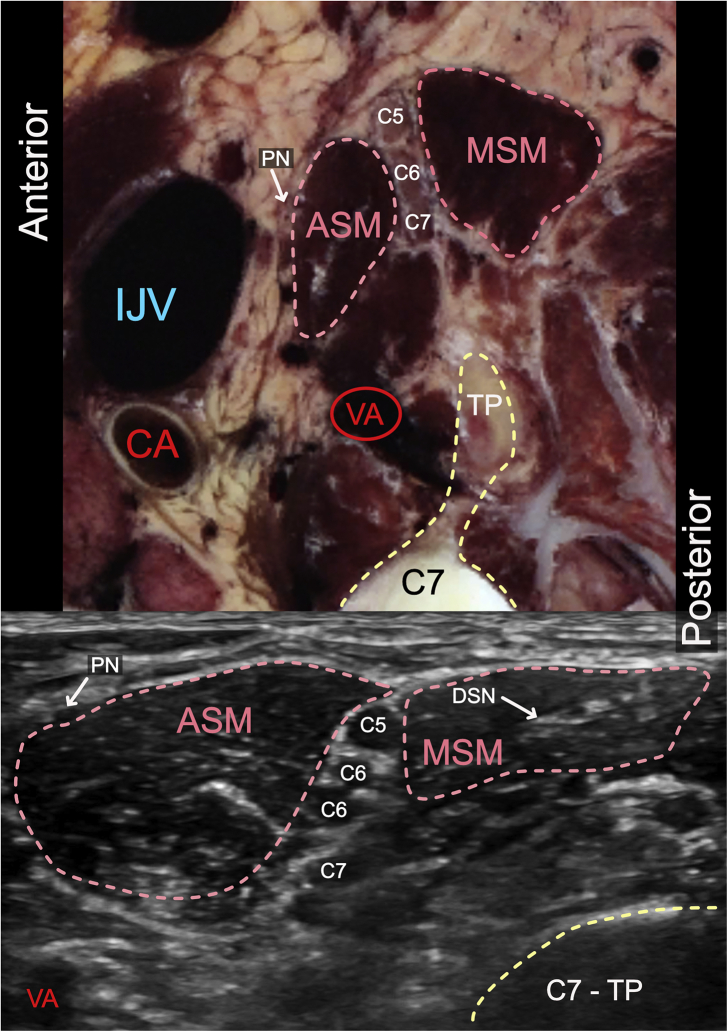
Cross-sectional and ultrasound interscalene brachial plexus anatomy (right arm). The roots are seen in the interscalene groove between the middle scalene muscle (MSM) and the anterior scalene muscle (ASM). The C6 root can commonly divide into two equally hypoechoic structures at this point on ultrasound. CA, carotid artery; DSN, dorsal scapular nerve; IJV, internal jugular vein; TP, transverse process of C7; VA, vertebral artery. The likely positions of the phrenic nerve (PN) are marked.

Schematic diagram showing the common locations of the nerves around the axillary artery (AA). The orientations are in relation to the AA as if the patient's left arm was slightly abducted. Viewing it like a clock face, the most common locations are median nerve (M) positioned at 11–12 (81%), ulnar nerve (U) at 2–3 (85%), and the radial nerve (R) at 4–6 (89%). The musculocutaneous nerve (Mc) is found laterally between the biceps brachii (BB) and coracobrachialis (CB) muscles at 8–9 (90%).

Cross-sectional view of left axillary fossa with corresponding ultrasound image. The axillary artery (AA) and axillary veins (AV) are enclosed within adipose tissue. BB, biceps brachii; CB, coracobrachialis muscle; McN, musculocutaneous nerve; MN, median nerve; RN, radial nerve; UN, ulnar nerve.

Schematic representation of the ulnar nerve route through the arm and forearm.

Cross-sectional view of right antecubital fossa with ultrasound image. The ulnar nerve (UN) is visible behind the medial epicondyle. The median nerve (MN) is medial to the brachial artery (BA), whilst the radial nerve is found between the brachioradialis muscle (BRM) and brachialis muscle (BM). PT, pronator teres muscle; RN, radial nerve.
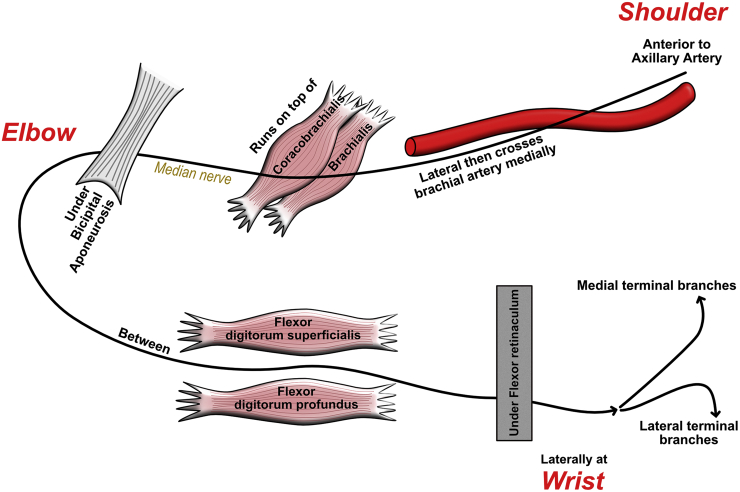
Schematic representation of the median nerve route through the arm into the forearm.
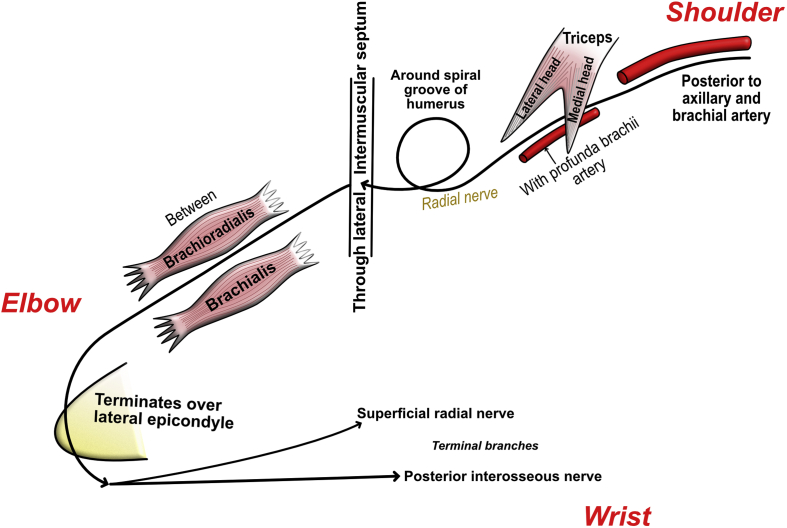
Schematic representation of the radial nerve route through the arm terminating at the lateral epicondyle.

Supraclavicular cross-section of brachial plexus with similar ultrasound image (right arm) - the probe is placed behind the clavicle (Cl), parallel to it initially then the lateral aspect of the probe is rotated posteriorly to optimise the image. This gives an oblique ultrasound view of the plexus and the first rib and is why it appears more compact. The brachial plexus (BP) is seen in relation to the subclavian artery (SA). With permission from Anatomage, Inc.

Infraclavicular brachial plexus cross-section with concurrent ultrasound view (right arm). The brachial plexus (medial cord - MC, posterior cord - PC and lateral cord - LC) can be seen surrounding the axillary artery (AA) with the axillary vein (AV). The plexus lies below the fascia (orange line) of the pectorals minor muscle (PMinM); PMajM - pectoralis major muscle.

Cross-sectional view of the humerus as the radial nerve (RN) leaves the spiral groove accompanying the profunda brachii artery (PB) with concurrent sonoanatomy (right arm). MN - Median nerve; BB - Biceps Brachii; TM - Triceps muscle; BA - Brachial Artery.
References
-
- Little D.M. Classical file. Survey Anesthesiol. 1963;7:280–285.
-
- Lalkhen A.G., Bhatia K. Perioperative peripheral nerve injuries. Cont Educ Anaesth Crit Care Pain. 2012;12:38–42.
-
- Neal J.M., Hebl J.R., Gerancher J.C., Hogan Q.H. Brachial plexus anesthesia: essentials of our current understanding. Reg Anesth Pain Med. 2002;27:402–428. - PubMed
-
- Hewson D.W., Bedforth N.M., Hardman J.G. Peripheral nerve injury arising in anaesthesia practice. Anaesthesia. 2018;73:51–60. - PubMed
-
- Rolak L.A. Mosby Elsevier; Philadelphia, PA: 2010. Neurology secrets.
Publication types
LinkOut - more resources
Full Text Sources
