

Multiple Spinal CSF Leaks in Spontaneous Intracranial Hypotension: Do They Exist?
- PMID: 34840885
- PMCID: PMC8610520
- DOI: 10.1212/CPJ.0000000000001084
Multiple Spinal CSF Leaks in Spontaneous Intracranial Hypotension: Do They Exist?
Abstract
Objective: To determine the frequency of multiple spinal CSF leaks in a recent group of patients with spontaneous intracranial hypotension (SIH) who were investigated with digital subtraction myelography (DSM).
Methods: This observational study was conducted using data from a prospectively maintained data base of patients who meet the International Classification of Headache Disorders, third edition, criteria for SIH. The patient population consisted of a consecutive group of 745 patients with SIH who underwent DSM between March 2009 and February 2020. Based on the results of DSM, participants were classified according to the type and number of spinal CSF leaks.
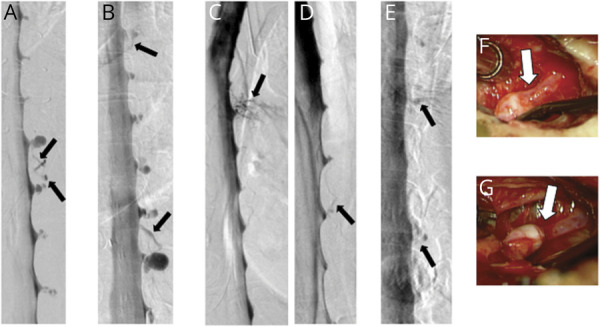
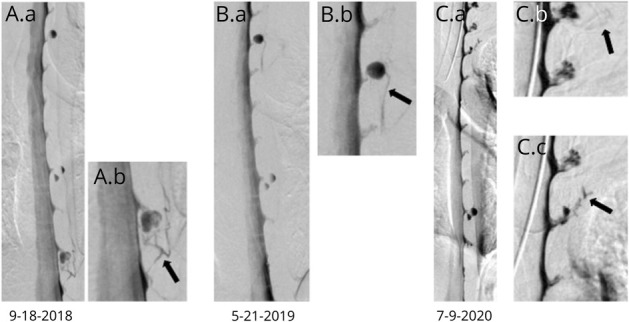
Results: Among 398 patients with SIH and extradural CSF on spinal imaging, multiplicity of CSF leaks was observed in none of 291 patients with type 1a ventral leaks and in 4 (6.2%) of 65 patients with type 1b (postero-) lateral leaks. Among 97 patients with SIH from spinal CSF-venous fistulas (type 3 leaks) who did not have extradural CSF on spinal imaging, 9 patients (9.3%) had multiple fistulas (p < 0.0001 for comparison between groups). Type 3 and type 1a or 1b CSF leaks coexisted in an additional 5 patients.
Conclusions: Among patients with SIH, multiplicity of CSF leaks was observed radiographically in none of the patients with ventral leaks, in 6% of patients with lateral leaks, and in 9% of patients with CSF-venous fistulas. These results suggest that patients with SIH can be reassured that the occurrence of multiple CSF leaks is negligible to uncommon at most, depending on the type of CSF leak.
© 2021 American Academy of Neurology.
Figures

References
-
- Mokri B. Spontaneous cerebrospinal fluid leaks: from intracranial hypotension to cerebrospinal fluid hypovolemia—evolution of a concept. Mayo Clin Proc. 1999;74(11):1113-1123. - PubMed
-
- Schievink WI. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. JAMA. 2006;295(19):2286-2296. - PubMed
-
- Rahman M, Bidari SS, Quisling RG, Friedman WA. Spontaneous intracranial hypotension: dilemmas in diagnosis. Neurosurgery. 2011;69(1):4-14. - PubMed
-
- Mokri B. Spontaneous intracranial hypotension. Continuum (Minneap Minn). 2015;21(4 headache):1086-1108. - PubMed
-
- Amrhein TJ, Kranz PG. Spontaneous intracranial hypotension: imaging in diagnosis and treatment. Radiol Clin North Am. 2019;57(2):439-451. - PubMed
LinkOut - more resources
Full Text Sources