

Risk of Fracture Among Older Adults With Primary Hyperparathyroidism Receiving Parathyroidectomy vs Nonoperative Management
- PMID: 34842909
- PMCID: PMC8630642
- DOI: 10.1001/jamainternmed.2021.6437
Risk of Fracture Among Older Adults With Primary Hyperparathyroidism Receiving Parathyroidectomy vs Nonoperative Management
Abstract
Importance: Primary hyperparathyroidism (PHPT) contributes to the development and progression of osteoporosis in older adults. The effectiveness of parathyroidectomy for reducing fracture risk in older adults is unknown.
Objective: To compare the incidence of clinical fracture among older adults with PHPT treated with parathyroidectomy vs nonoperative management.
Design, setting, and participants: This was a population-based, longitudinal cohort study of all Medicare beneficiaries with PHPT from 2006 to 2017. Multivariable, inverse probability weighted Cox proportional hazards and Fine-Gray competing risk regression models were constructed to determine the association of parathyroidectomy vs nonoperative management with incident fracture. Data analysis was conducted from February 17, 2021, to September 14, 2021.
Main outcomes and measures: The primary outcome was clinical fracture at any anatomic site not associated with major trauma during the follow-up period.
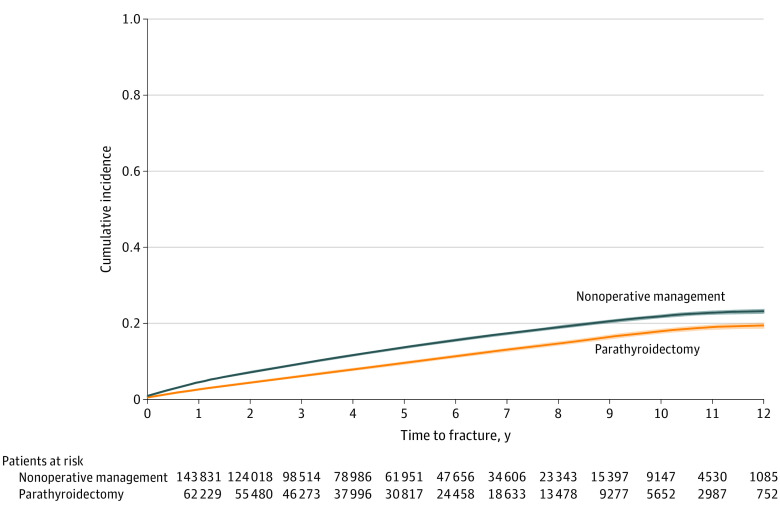
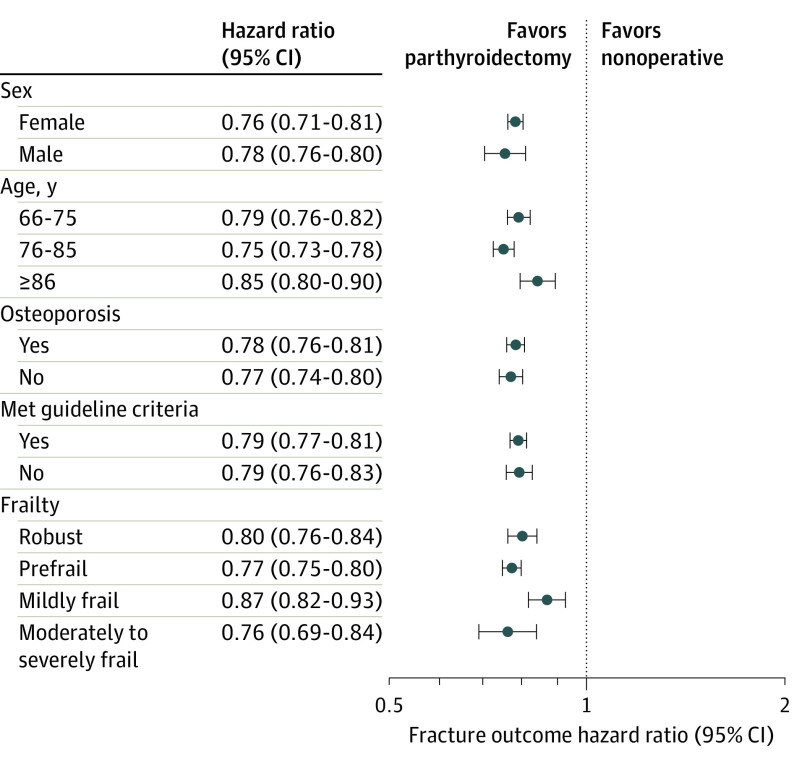
Results: Among the 210 206 Medicare beneficiaries with PHPT (mean [SD] age, 75 [6.8] years; 165 637 [78.8%] women; 183 433 [87.3%] White individuals), 63 136 (30.0%) underwent parathyroidectomy within 1 year of diagnosis, and 147 070 (70.0%) were managed nonoperatively. During a mean (SD) follow-up period of 58.5 (35.5) months, the unadjusted incidence of fracture was 10.2% in patients treated with parathyroidectomy. During a mean (SD) follow-up of 52.5 (33.8) months, the unadjusted incidence of fracture was 13.7% in patients observed nonoperatively. On multivariable analysis, parathyroidectomy was associated with lower adjusted rates of any fracture (hazard ratio [HR], 0.78; 95% CI, 0.76-0.80]) and hip fracture (HR, 0.76; 95% CI, 0.72-0.79). At 2, 5, and 10 years, parathyroidectomy was associated with adjusted absolute fracture risk reduction of 1.2% (95% CI, 1.0-1.4), 2.8% (95% CI, 2.5-3.1), and 5.1% (95% CI, 4.6-5.5), respectively, compared with nonoperative management. On subgroup analysis, there were no significant differences in the association of parathyroidectomy with fracture risk by age group, sex, frailty, history of osteoporosis, or meeting operative guidelines. Fine-Gray competing risk regression confirmed parathyroidectomy was associated with a lower probability of any fracture and hip fracture when accounting for the competing risk of death (HR, 0.84; 95% CI, 0.82-0.85; and HR, 0.83; 95% CI, 0.80-0.85, respectively).
Conclusions and relevance: This longitudinal cohort study found that parathyroidectomy was associated with a lower risk of any fracture and hip fracture among older adults with PHPT, suggesting a clinically meaningful benefit of operative management in this population.
Conflict of interest statement
Figures
Comment in
-
Parathyroidectomy in Elderly Individuals With Primary Hyperparathyroidism: To Operate or Not to Operate.JAMA Intern Med. 2022 Jan 1;182(1):7-8. doi: 10.1001/jamainternmed.2021.6816. JAMA Intern Med. 2022. PMID: 34842895 No abstract available.
References
-
- Coker LH, Rorie K, Cantley L, et al. . Primary hyperparathyroidism, cognition, and health-related quality of life. Ann Surg. 2005;242(5):642-650. doi:10.1097/01.sla.0000186337.83407.ec - DOI - PMC - PubMed
