

Antiseizure Medication Treatment and Outcomes in Patients with Subarachnoid Hemorrhage Undergoing Continuous EEG Monitoring
- PMID: 34843082
- PMCID: PMC9117405
- DOI: 10.1007/s12028-021-01387-x
Antiseizure Medication Treatment and Outcomes in Patients with Subarachnoid Hemorrhage Undergoing Continuous EEG Monitoring
Abstract
Background: Patients with aneurysmal subarachnoid hemorrhage (aSAH) with electroencephalographic epileptiform activity (seizures, periodic and rhythmic patterns, and sporadic discharges) are frequently treated with antiseizure medications (ASMs). However, the safety and effectiveness of ASM treatment for epileptiform activity has not been established. We used observational data to investigate the effectiveness of ASM treatment in patients with aSAH undergoing continuous electroencephalography (cEEG) to develop a causal hypothesis for testing in prospective trials.
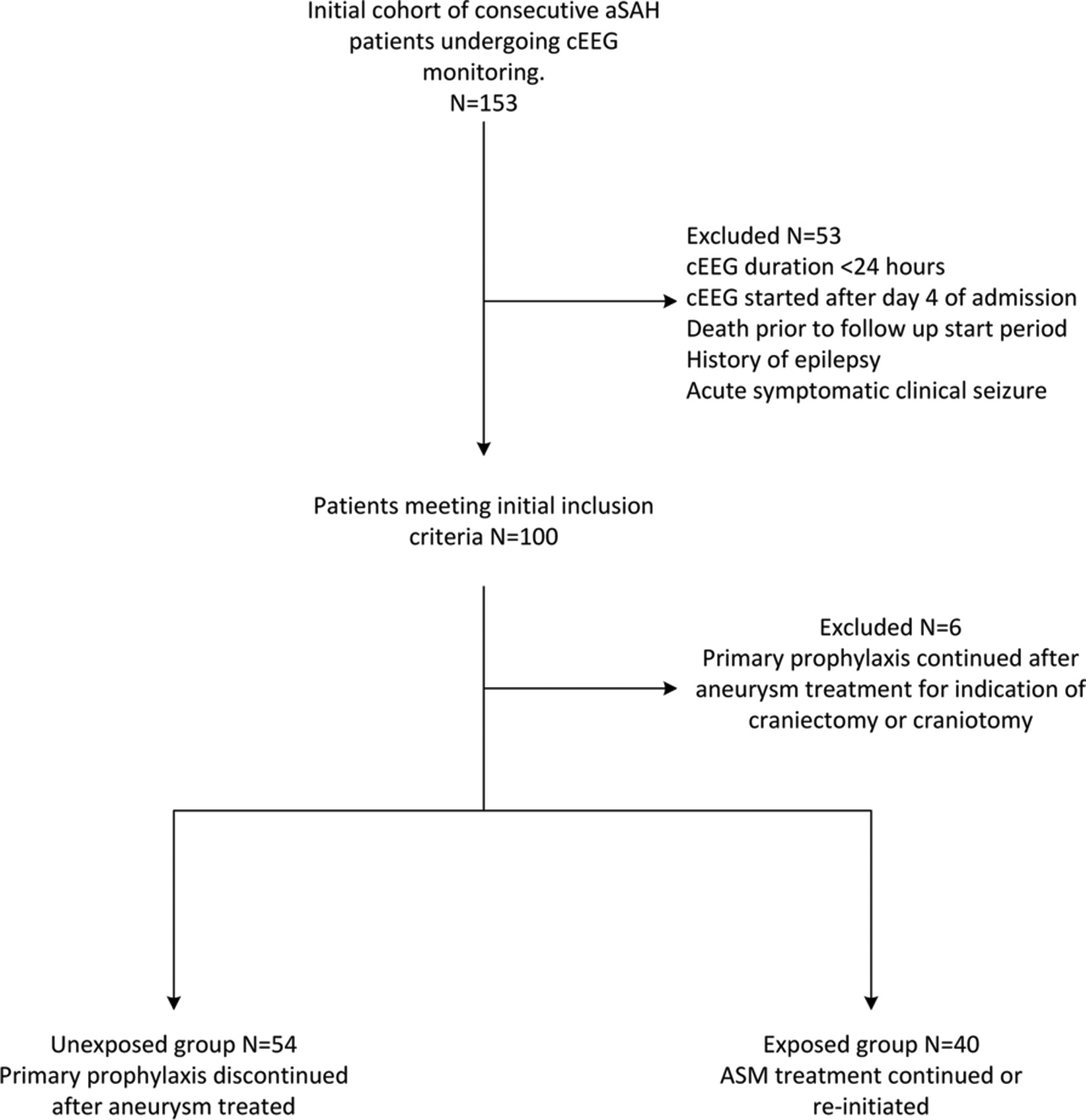
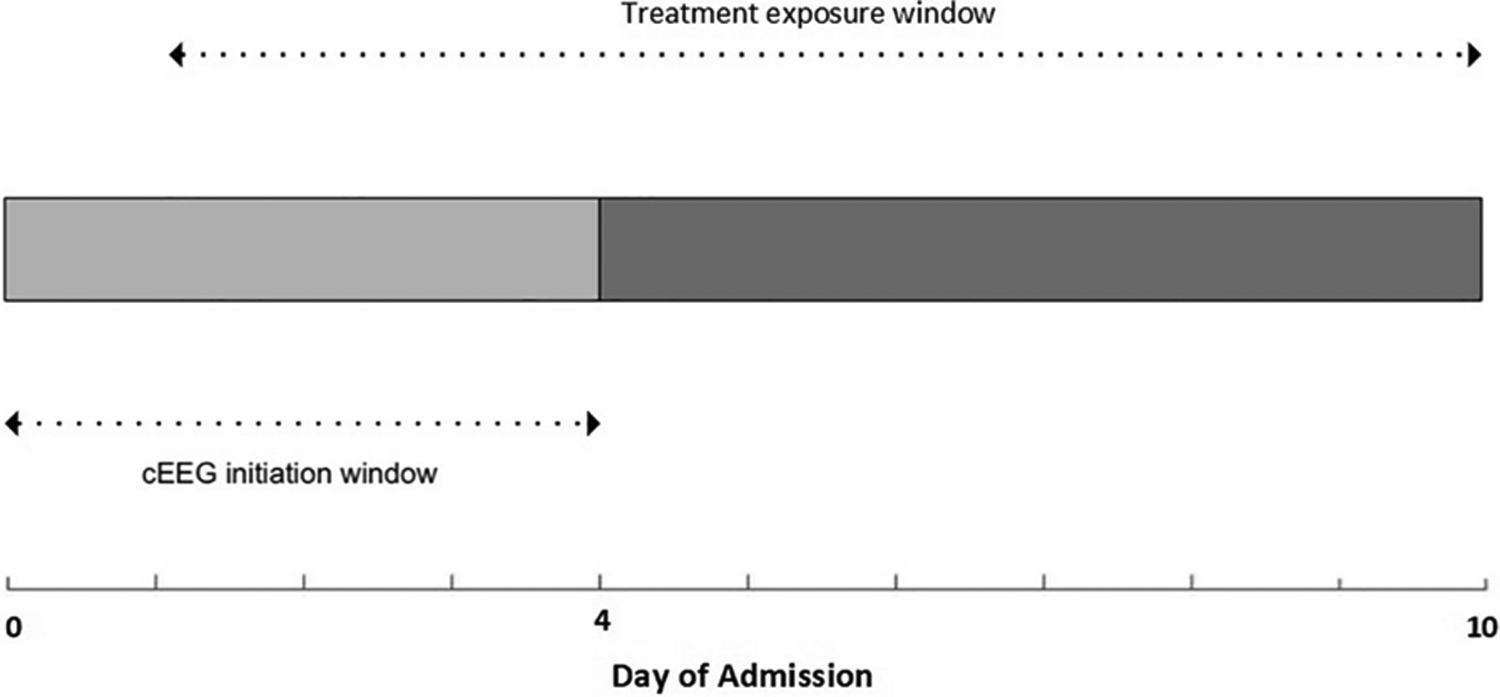
Methods: This was a retrospective single-center cohort study of patients with aSAH admitted between 2011 and 2016. Patients underwent ≥ 24 h of cEEG within 4 days of admission. All patients received primary ASM prophylaxis until aneurysm treatment (typically within 24 h of admission). Treatment exposure was defined as reinitiation of ASMs after aneurysm treatment and cEEG initiation. We excluded patients with non-cEEG indications for ASMs (e.g., epilepsy, acute symptomatic seizures). Outcomes measures were 90-day mortality and good functional outcome (modified Rankin Scale scores 0-3). Propensity scores were used to adjust for baseline covariates and disease severity.
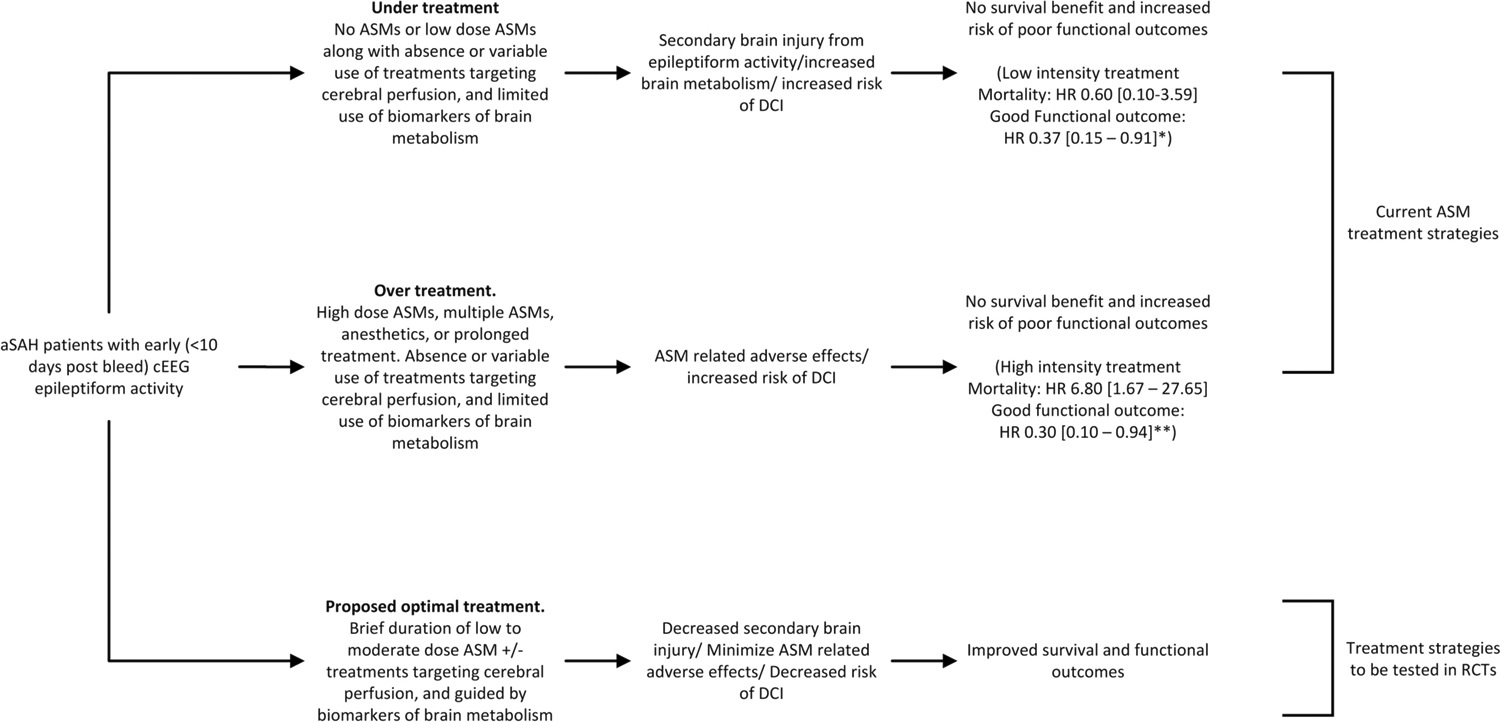
Results: Ninety-four patients were eligible (40 continued ASM treatment; 54 received prophylaxis only). ASM continuation was not significantly associated with higher 90-day mortality (propensity-adjusted hazard ratio [HR] = 2.01 [95% confidence interval (CI) 0.57-7.02]). ASM continuation was associated with lower likelihood for 90-day good functional outcome (propensity-adjusted HR = 0.39 [95% CI 0.18-0.81]). In a secondary analysis, low-intensity treatment (low-dose single ASM) was not significantly associated with mortality (propensity-adjusted HR = 0.60 [95% CI 0.10-3.59]), although it was associated with a lower likelihood of good outcome (propensity-adjusted HR = 0.37 [95% CI 0.15-0.91]), compared with prophylaxis. High-intensity treatment (high-dose single ASM, multiple ASMs, or anesthetics) was associated with higher mortality (propensity-adjusted HR = 6.80 [95% CI 1.67-27.65]) and lower likelihood for good outcomes (propensity-adjusted HR = 0.30 [95% CI 0.10-0.94]) compared with prophylaxis only.
Conclusions: Our findings suggest the testable hypothesis that continuing ASMs in patients with aSAH with cEEG abnormalities does not improve functional outcomes. This hypothesis should be tested in prospective randomized studies.
Keywords: Anticonvulsants; Electroencephalography; Outcome assessment; Seizures; Subarachnoid hemorrhage.
© 2021. Springer Science+Business Media, LLC, part of Springer Nature and Neurocritical Care Society.
Figures
Low intensity treatment: Monotherapy with: levetiracetam at a dose of <2000mg/day (<1000mg/day in impaired renal function), phenytoin at ≤ 300mg/day or mean level < 15mcg/mL, valproic acid at ≤ 15mg/kg/day or mean level < 75mcg/mL, or lacosamide at ≤ 200mg/day
High intensity treatment: >48 hours of levetiracetam at doses of ≥ 2000mg/day (≥ 1000mg/day in impaired renal function), phenytoin at >300mg/day or mean level ≥ 15mcg/mL, Valproic acid at >15mg/kg/day or mean level ≥ 75mcg/mL, lacosamide > 200mg/day, use of 2 or more ASMs, or initiation of anesthetics for treatment of epileptiform activity.
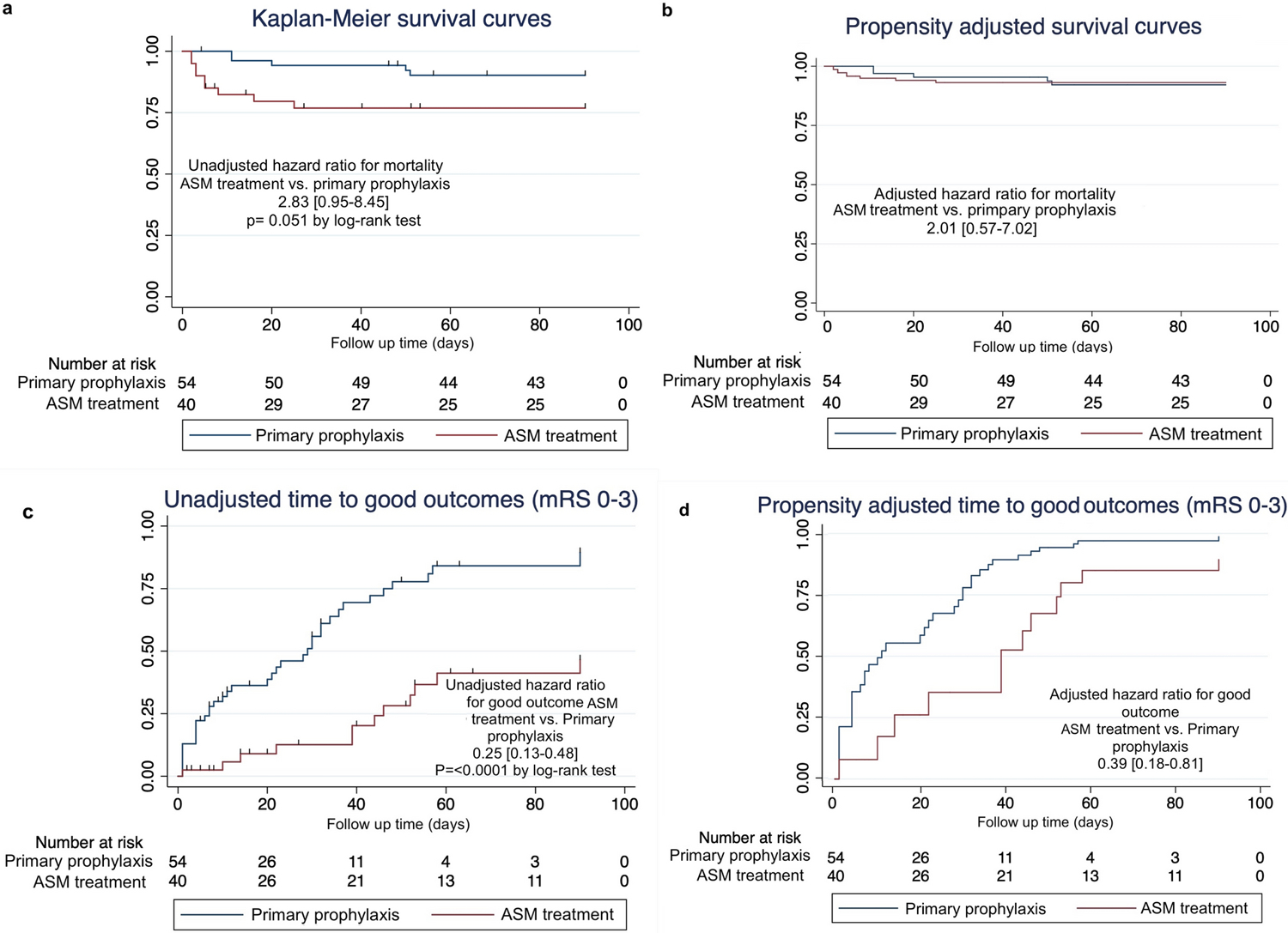
Kaplan-Meier curves for time to death comparing ASM treatment (low + high intensity) vs. prophylaxis only.
Propensity score adjusted survival curves for time to death comparing ASM treatment (low + high intensity) vs. prophylaxis only.
Kaplan-Meier curves for time to good functional outcome (mRS 0–3) comparing ASM treatment (low+ high intensity) vs. prophylaxis only.
Propensity score adjusted survival curves for time to good functional outcome (mRS 0–3) comparing ASM treatment (low+ high intensity) vs. prophylaxis only.
References
-
- Claassen J, Hirsch LJ, Frontera JA, Fernandez A, Schmidt M, Kapinos G, Wittman J, et al. Prognostic significance of continuous EEG monitoring in patients with poor-grade subarachnoid hemorrhage. Neurocrit Care. 2006;4:103–12. - PubMed
-
- Naidech AM, Kreiter KT, Janjua N, Ostapkovich N, Parra A, Commichau C, Connolly ES, et al. Phenytoin exposure is associated with functional and cognitive disability after subarachnoid hemorrhage. Stroke. 2005;36:583–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
