

Small airway dysfunction on impulse oscillometry and pathological signs on lung ultrasound are frequent in post-COVID-19 patients with persistent respiratory symptoms
- PMID: 34843598
- PMCID: PMC8629296
- DOI: 10.1371/journal.pone.0260679
Small airway dysfunction on impulse oscillometry and pathological signs on lung ultrasound are frequent in post-COVID-19 patients with persistent respiratory symptoms
Abstract
Background: Thousands of people worldwide are suffering the consequences of coronavirus disease-2019 (COVID-19), and impulse oscillometry (IOS) and lung ultrasound (LUS) might be important tools for the follow-up of this population. Our objective was to prospectively evaluate abnormalities detected using these two methods in a cohort of COVID-19 survivors with respiratory symptoms.
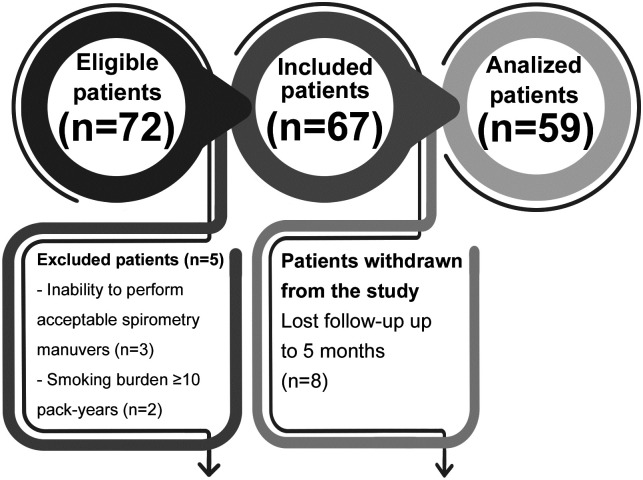
Methods: In this follow-up study, 59 patients underwent clinical evaluations, spirometry, IOS and LUS in the 2nd (M1) and 5th (M2) months after diagnostic confirmation of COVID-19 by real-time reverse transcriptase-polymerase chain reaction. Aeration scores were obtained from the LUS exams based on the following findings: B-lines >2, coalescent B-lines, and subpleural consolidations.
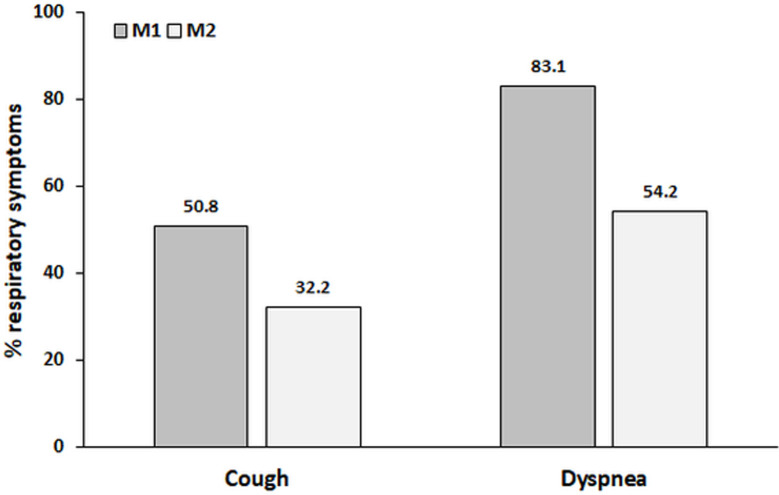
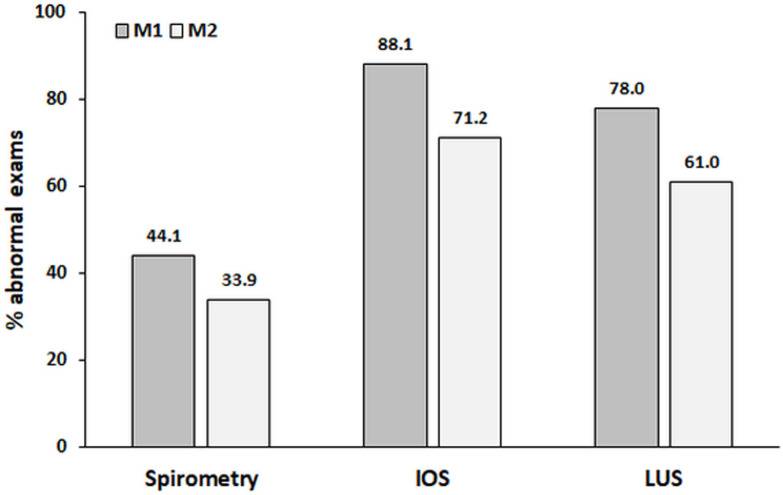
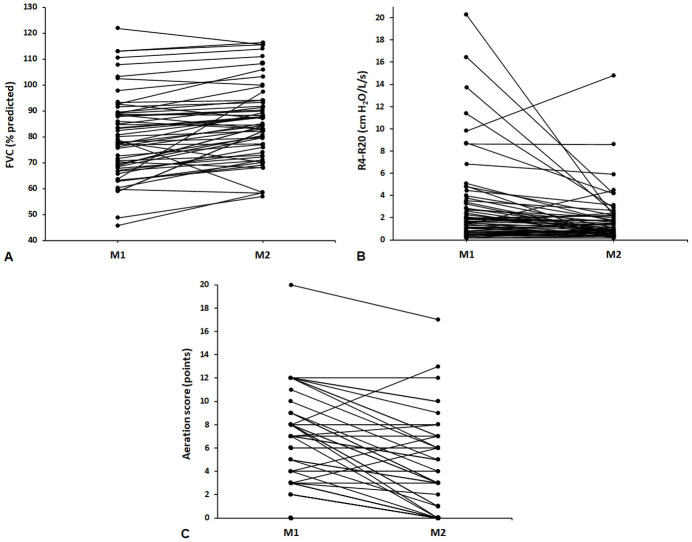
Results: Fifty-nine (100%) participants had cough and/or dyspnea at M1, which decreased to 38 (64.4%) at M2 (p = 0.0001). Spirometry was abnormal in 26 (44.1%) and 20 (33.9%) participants at M1 and M2, respectively, although without statistical significance (p = 0.10). Normal examination, restrictive patterns, and obstructive patterns were observed in 33 (55.9%), 18 (30.5%), and 8 (13.6%) participants, respectively, at M1 and in 39 (66.1%), 13 (22%), and 7 (11.9%) participants at M2 (p = 0.14). Regarding IOS, considering changes in resistive and reactive parameters, abnormal exams were detected in 52 (88.1%) and 42 (71.2%) participants at M1 and M2, respectively (p = 0.002). Heterogeneity of resistance between 4 and 20 Hz >20% was observed in 38 (64.4%) and 33 (55.9%) participants at M1 and M2, respectively (p = 0.30). Abnormal LUS was observed in 46 (78%) and 36 (61%) participants at M1 and M2, respectively (p = 0.002), with a reduction in aeration scores between M1 and M2 [5 (2-8) vs. 3 (0-6) points, p<0.0001].
Conclusions: IOS and LUS abnormalities are frequent in the first 5 months post-COVID-19 infection; however, when prospectively evaluated, significant improvement is evident in the parameters measured by these two methods.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
