

Cellular and humoral immunogenicity of the mRNA-1273 SARS-CoV-2 vaccine in patients with hematologic malignancies
- PMID: 34844263
- PMCID: PMC8632354
- DOI: 10.1182/bloodadvances.2021006101
Cellular and humoral immunogenicity of the mRNA-1273 SARS-CoV-2 vaccine in patients with hematologic malignancies
Abstract
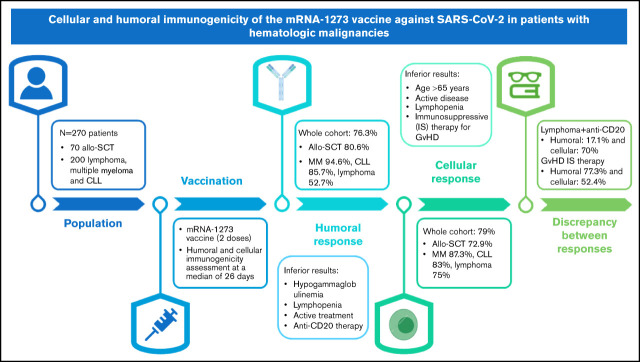
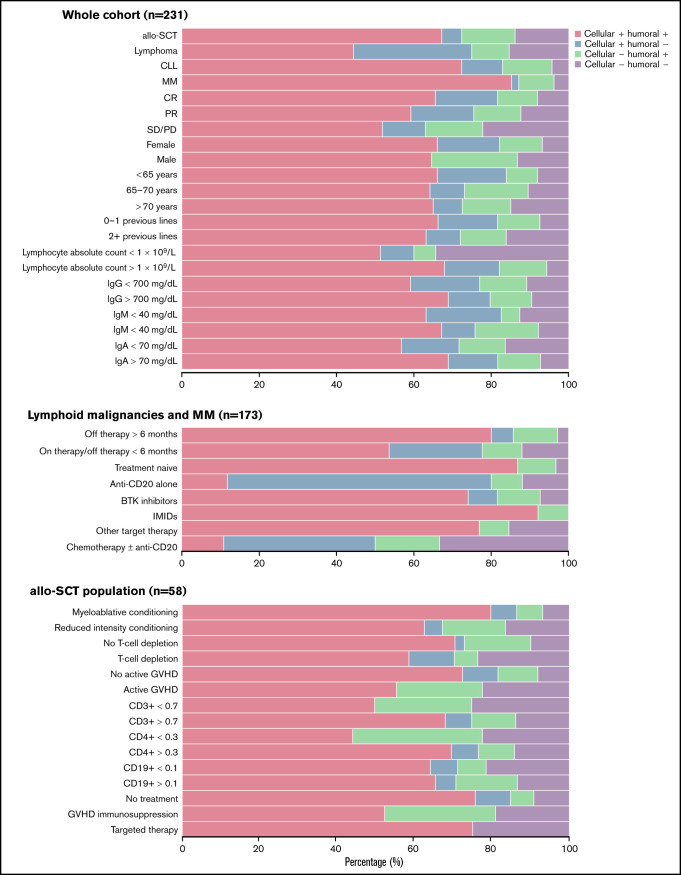
Recent studies have shown a suboptimal humoral response to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) messenger RNA (mRNA) vaccines in patients diagnosed with hematologic malignancies; however, data about cellular immunogenicity are scarce. The aim of this study was to evaluate both the humoral and cellular immunogenicity 1 month after the second dose of the mRNA-1273 vaccine. Antibody titers were measured by using the Elecsys and LIAISON anti-SARS-CoV-2 S assays, and T-cell response was assessed by using interferon-γ release immunoassay technology. Overall, 76.3% (184 of 241) of patients developed humoral immunity, and the cellular response rate was 79% (184 of 233). Hypogammaglobulinemia, lymphopenia, active hematologic treatment, and anti-CD20 therapy during the previous 6 months were associated with an inferior humoral response. Conversely, age >65 years, active disease, lymphopenia, and immunosuppressive treatment of graft-versus-host disease (GVHD) were associated with an impaired cellular response. A significant dissociation between the humoral and cellular responses was observed in patients treated with anti-CD20 therapy (the humoral response was 17.5%, whereas the cellular response was 71.1%). In these patients, B-cell aplasia was confirmed while T-cell counts were preserved. In contrast, humoral response was observed in 77.3% of patients undergoing immunosuppressive treatment of GVHD, whereas only 52.4% had a cellular response. The cellular and humoral responses to the SARS-CoV-2 mRNA-1273 vaccine in patients with hematologic malignancies are highly influenced by the presence of treatments such as anti-CD20 therapy and immunosuppressive agents. This observation has implications for the further management of these patients.
© 2022 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Figures



References
-
- Passamonti F, Cattaneo C, Arcaini L, et al. ; ITA-HEMA-COV Investigators . Clinical characteristics and risk factors associated with COVID-19 severity in patients with haematological malignancies in Italy: a retrospective, multicentre, cohort study. Lancet Haematol. 2020;7(10):e737-e745. - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
