

Fracture profiles of a 4-year cohort of 266,324 first incident upper extremity fractures from population health data in Ontario
- PMID: 34844604
- PMCID: PMC8630866
- DOI: 10.1186/s12891-021-04849-7
Fracture profiles of a 4-year cohort of 266,324 first incident upper extremity fractures from population health data in Ontario
Abstract
Background: Understanding the profiles of different upper extremity fractures, particularly those presenting as a 1st incident can inform prevention and management strategies. The purpose of this population-level study was to describe first incident fractures of the upper extremity in terms of fracture characteristics and demographics.
Methods: Cases with a first adult upper extremity (UE) fracture from the years 2013 to 2017 were extracted from administrative data in Ontario. Fracture locations (ICD-10 codes) and associated characteristics (open/closed, associated hospitalization within 1-day, associated nerve, or tendon injury) were described by fracture type, age category and sex. Standardized mean differences of at least 10% (clinical significance) and statistical significance (p < 0.01) in ANOVA were used to identify group differences (age/sex).
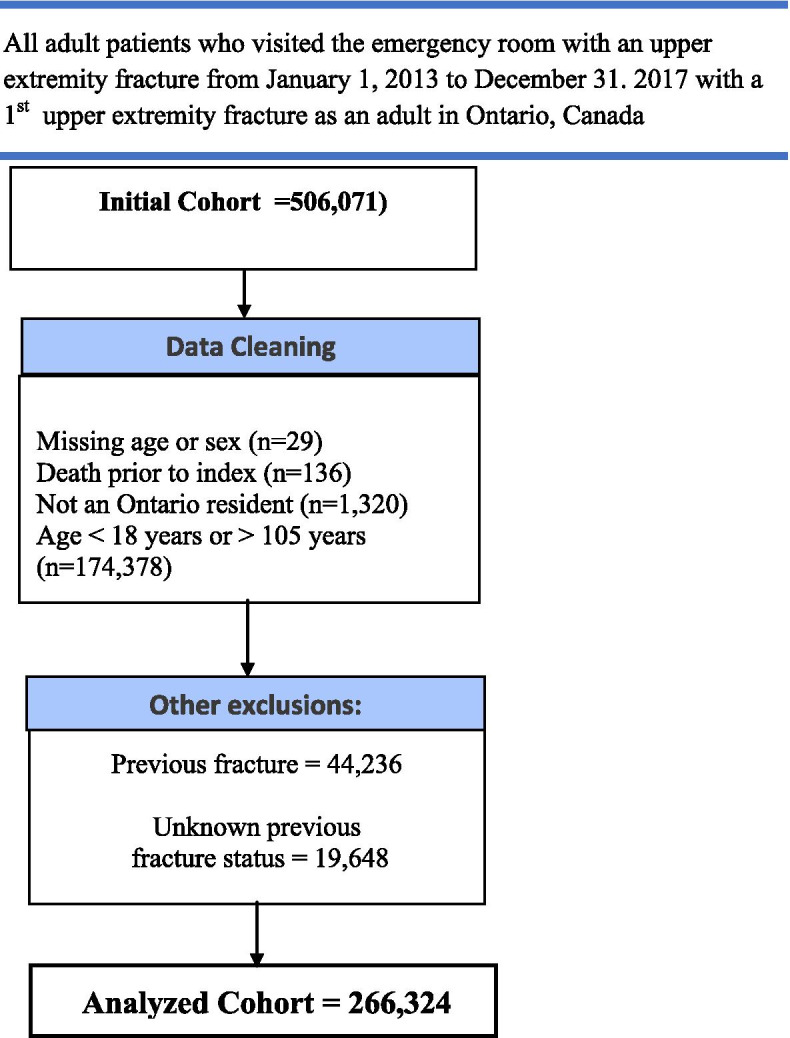
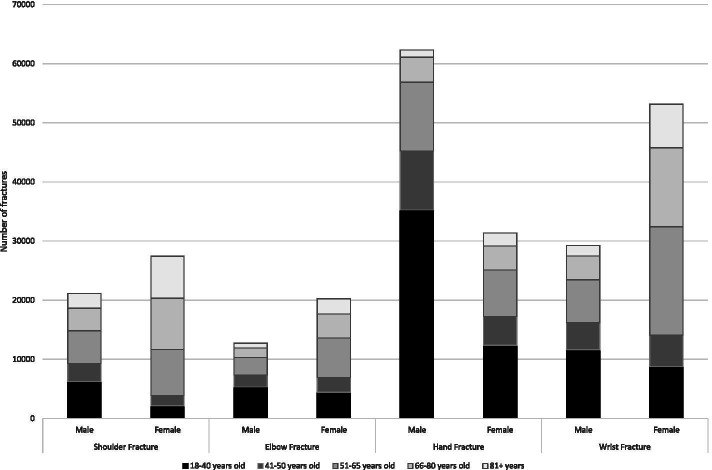
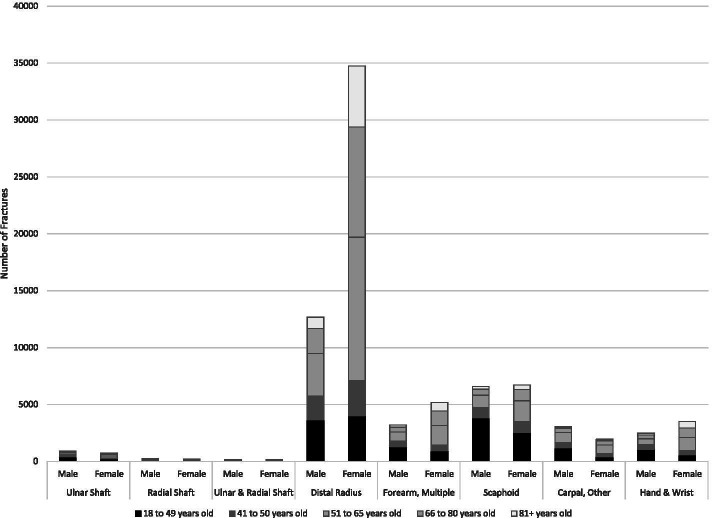
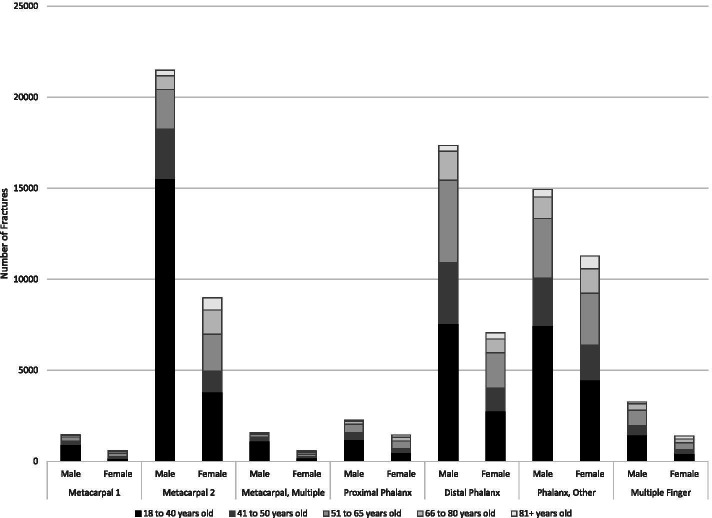
Results: We identified 266,324 first incident UE fractures occurring over 4 years. The most commonly affected regions were the hand (93 K), wrist/forearm(80 K), shoulder (48 K) or elbow (35 K). The highest number of specific fractures were: distal radius (DRF, 47.4 K), metacarpal (30.4 K), phalangeal (29.9 K), distal phalangeal (24.4 K), proximal humerus (PHF, 21.7 K), clavicle (15.1 K), radial head (13.9 K), and scaphoid fractures (13.2 K). The most prevalent multiple fractures included: multiple radius and ulna fractures (11.8 K), fractures occurring in multiple regions of the upper extremity (8.7 K), or multiple regions in the forearm (8.4 K). Tendon (0.6% overall; 8.2% in multiple finger fractures) or nerve injuries were rarely reported (0.3% overall, 1.5% in distal humerus). Fractures were reported as being open in 4.7% of cases, most commonly for distal phalanx (23%). A similar proportion of females (51.5%) and males were present in this fracture cohort, but there were highly variant age-sex profiles across fracture subtypes. Fractures most common in 18-40-year-old males included metacarpal and finger fractures. Fractures common in older females were: DRF, PHF and radial head, which exhibited a dramatic increase in the over-50 age group.
Conclusions: UE fracture profiles vary widely by fracture type. Fracture specific prevention and management should consider fracture profiles that are highly variable according to age and sex.
Keywords: Comorbidity; Distal radius; Epidemiology; Fractures; Nerve injury; Proximal humerus; Scaphoid; Sex differences; Social deprivation; Tendon injury; Upper extremity.
© 2021. The Author(s).
Conflict of interest statement
None.
Figures


References
-
- Ahmed LA, Schirmer ÆH, Jørgensen L, Størmer ÆJ, Joakimsen ÆRM. The gender- and age-specific 10-year and lifetime absolute fracture risk in Tromsø , Norway. 2009;:441–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
