

Nutritional risk factors for SARS-CoV-2 infection: a prospective study within the NutriNet-Santé cohort
- PMID: 34844606
- PMCID: PMC8629697
- DOI: 10.1186/s12916-021-02168-1
Nutritional risk factors for SARS-CoV-2 infection: a prospective study within the NutriNet-Santé cohort
Abstract
Background: Nutritional factors are essential for the functioning of the immune system and could therefore play a role in COVID-19 but evidence is needed. Our objective was to study the associations between diet and the risk of SARS-CoV-2 infection in a large population-based sample.
Methods: Our analyses were conducted in the French prospective NutriNet-Santé cohort study (2009-2020). Seroprevalence of anti-SARS-CoV-2 antibodies was assessed by ELISA on dried blood spots. Dietary intakes were derived from repeated 24 h dietary records (at least 6) in the two years preceding the start of the COVID-19 pandemic in France (February 2020). Multi-adjusted logistic regression models were computed.
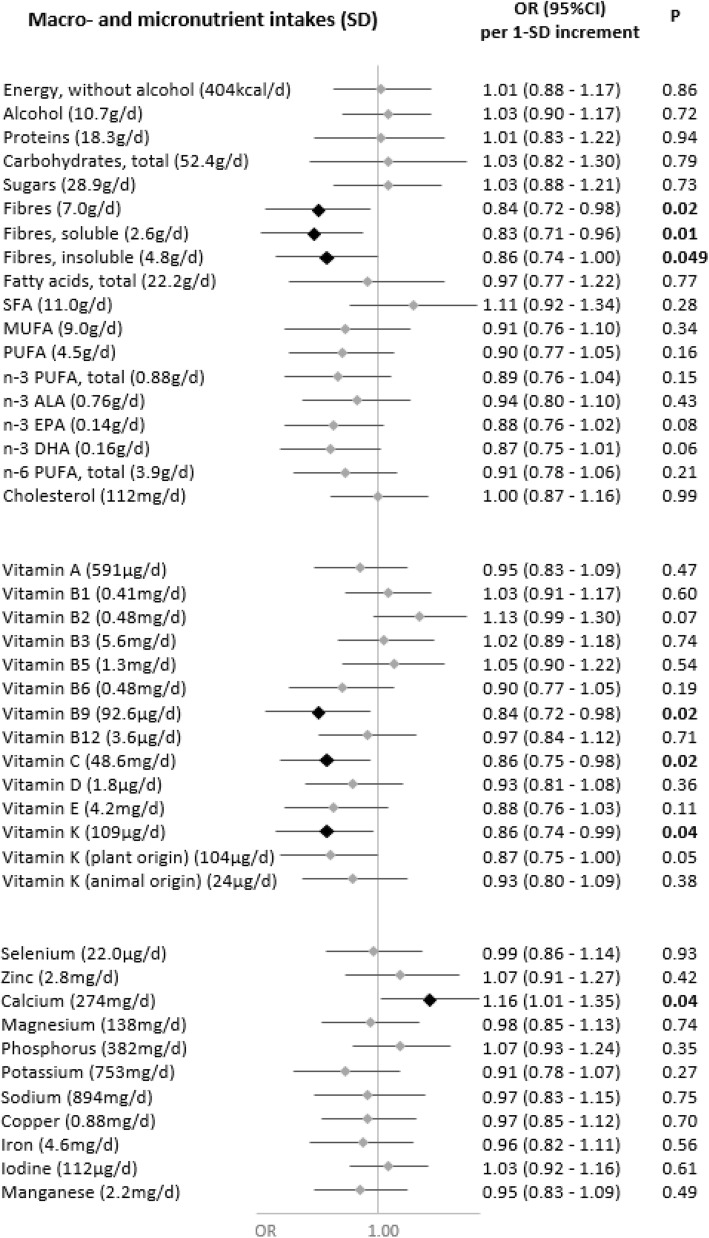
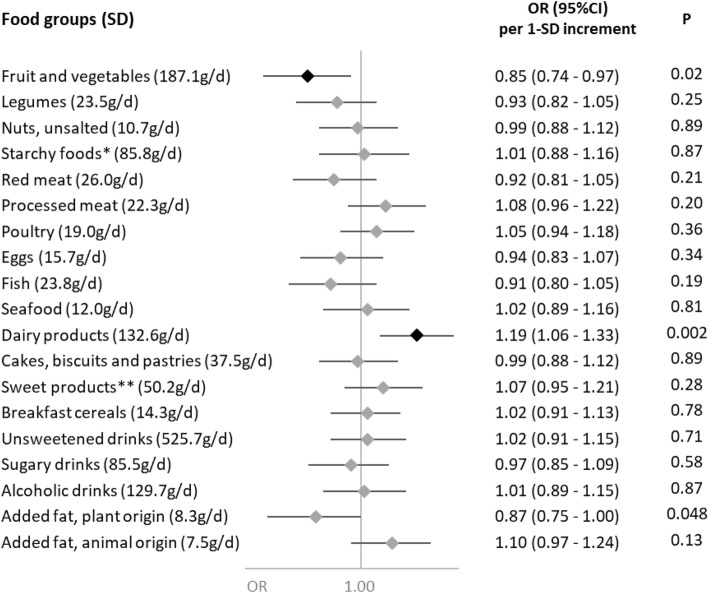
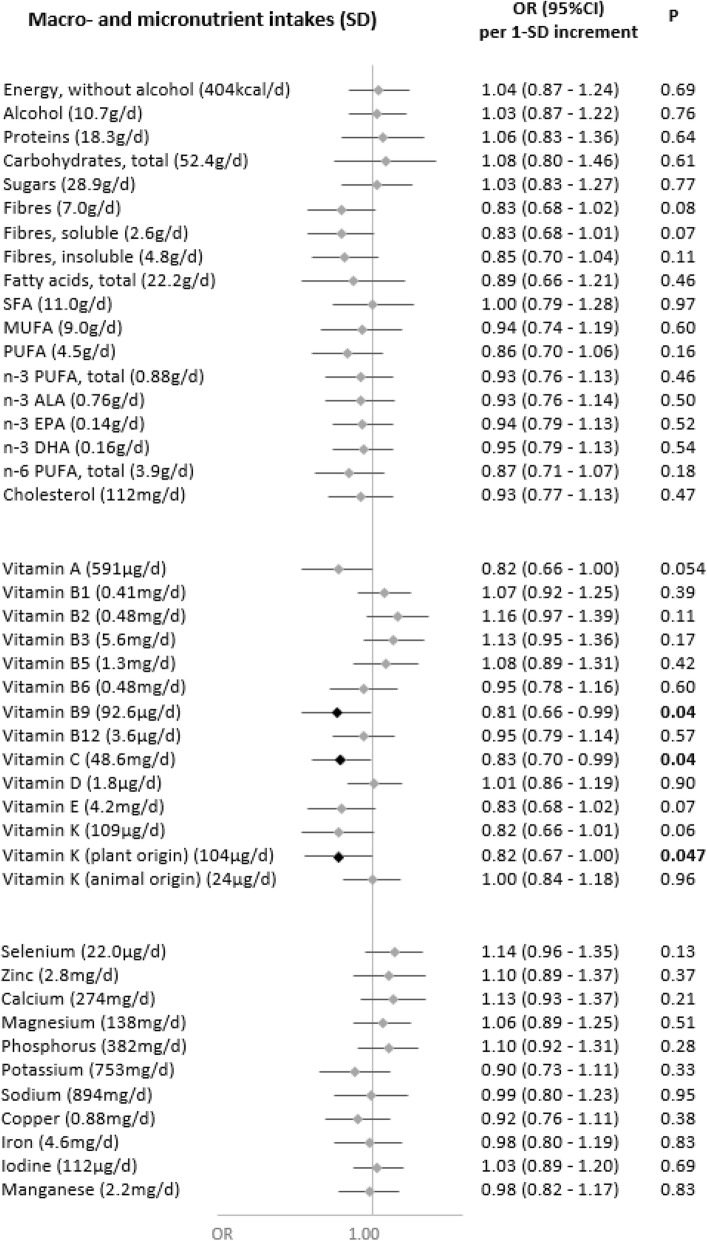
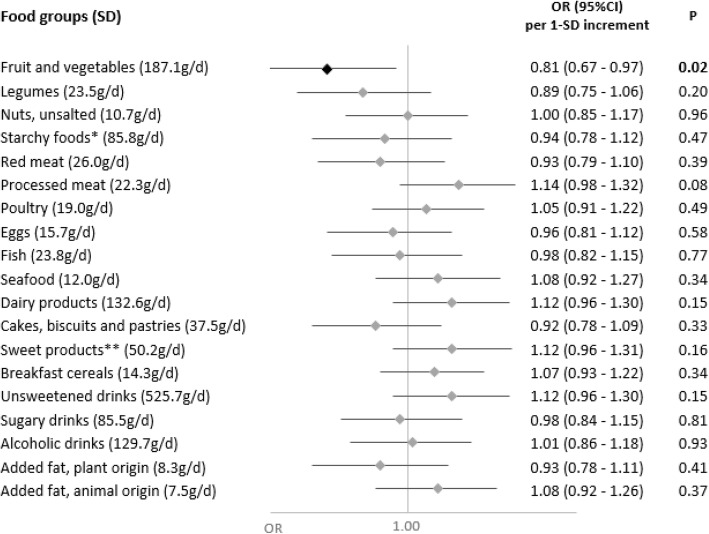
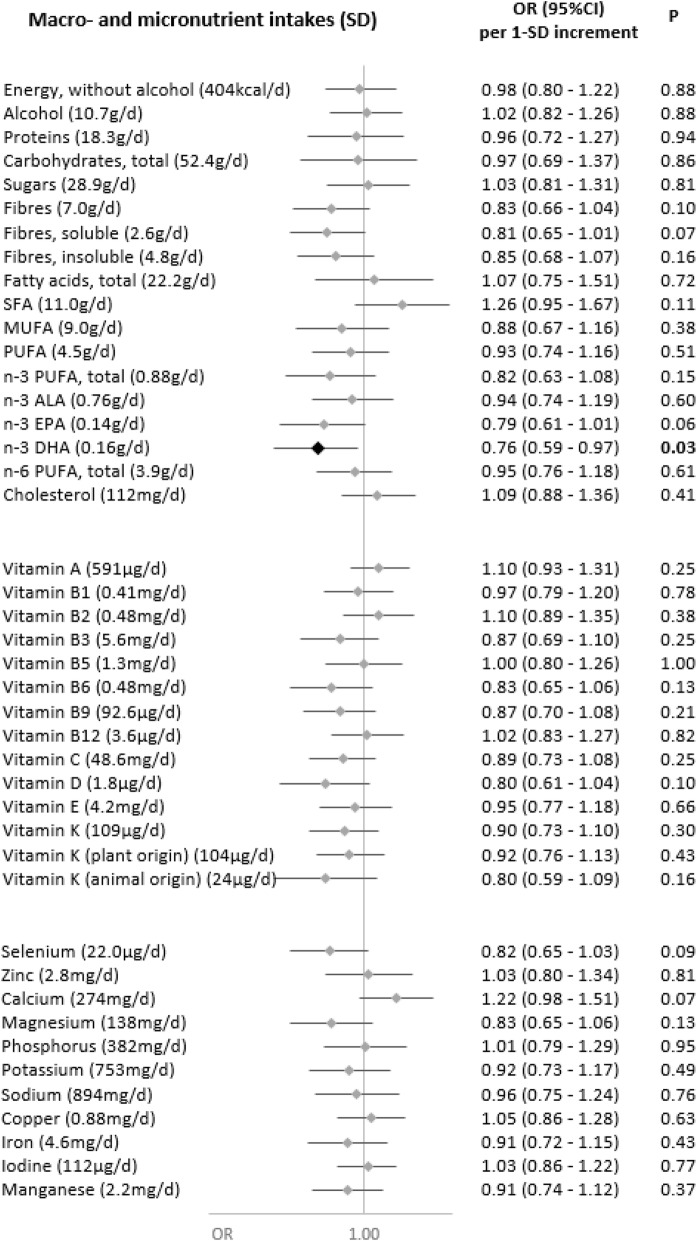
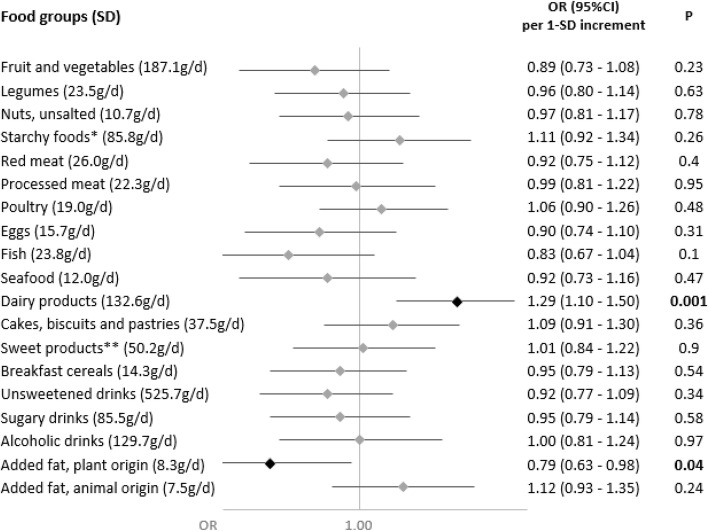
Results: A total of 7766 adults (70.3% women, mean age: 60.3 years) were included, among which 311 were positive for anti-SARS-CoV-2 antibodies. Dietary intakes of vitamin C (OR for 1 SD=0.86 (0.75-0.98), P=0.02), vitamin B9 (OR=0.84 (0.72-0.98), P=0.02), vitamin K (OR=0.86 (0.74-0.99), P=0.04), fibers (OR=0.84 (0.72-0.98), P=0.02), and fruit and vegetables (OR=0.85 (0.74-0.97), P=0.02) were associated to a decreased probability of SARS-CoV-2 infection while dietary intakes of calcium (OR=1.16 (1.01-1.35), P=0.04) and dairy products (OR=1.19 (1.06-1.33), P=0.002) associated to increased odds. No association was detected with other food groups or nutrients or with the overall diet quality.
Conclusions: Higher dietary intakes of fruit and vegetables and, consistently, of vitamin C, folate, vitamin K and fibers were associated with a lower susceptibility to SARS-CoV-2 infection. Beyond its established role in the prevention of non-communicable diseases, diet could therefore also contribute to prevent some infectious diseases such as COVID-19.
Trial registration: ClinicalTrials.gov NCT03335644.
Keywords: Cohort study; Diet; SARS-CoV-2; Seroprevalence; Vitamins.
© 2021. The Author(s).
Conflict of interest statement
Prof Fabrice Carrat reports personal fees from Imaxio and Sanofi, outside the submitted work. All other authors declare no competing interest.
Figures
References
-
- WHO. Coronavirus disease (COVID-19) pandemic. https://www.who.int/emergencies/diseases/novel-coronavirus-2019. Accessed 25 Sept 2021.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
