

Incidence of childhood cancer in Canada during the COVID-19 pandemic
- PMID: 34844937
- PMCID: PMC8654886
- DOI: 10.1503/cmaj.210659
Incidence of childhood cancer in Canada during the COVID-19 pandemic
Abstract
Background: The COVID-19 pandemic has had a major impact on access to health care resources. Our objective was to estimate the impact of the COVID-19 pandemic on the incidence of childhood cancer in Canada. We also aimed to compare the proportion of patients who enrolled in clinical trials at diagnosis, presented with metastatic disease or had an early death during the first 9 months of the COVID-19 pandemic compared with previous years.
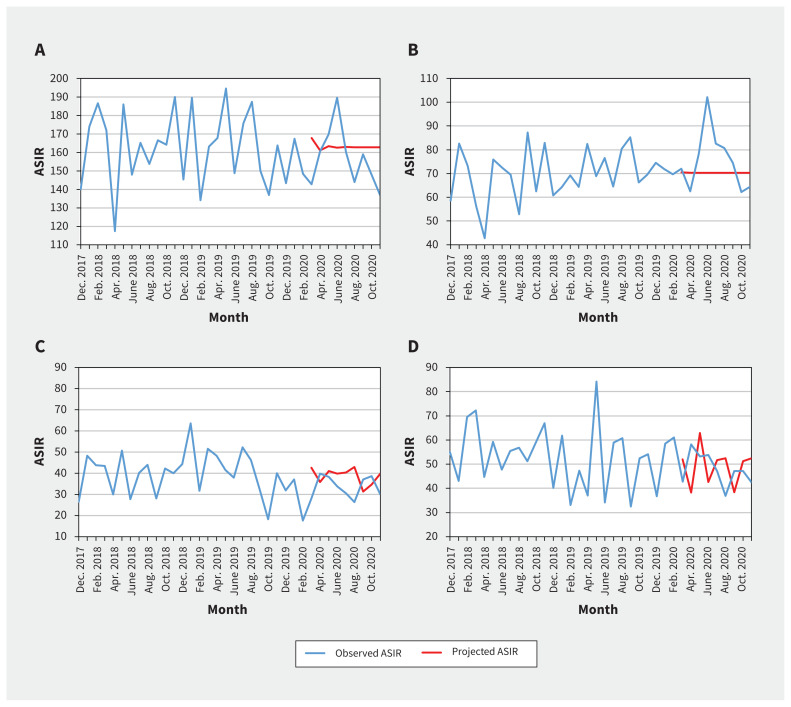
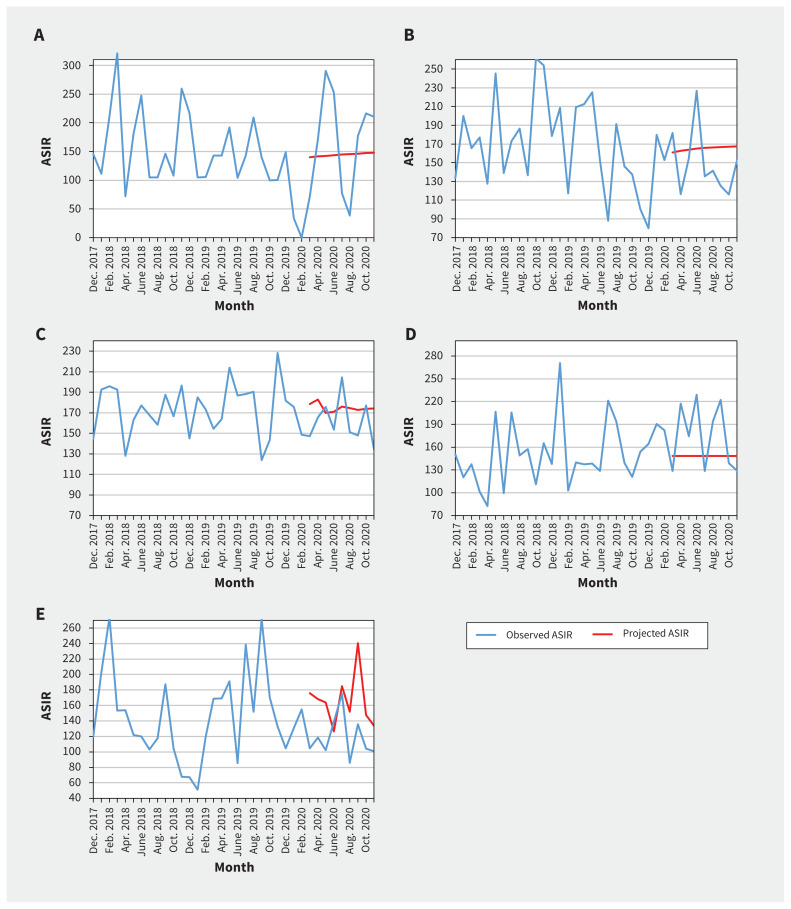
Methods: We conducted an observational study that included children younger than 15 years with a new diagnosis of cancer between March 2016 and November 2020 at 1 of 17 Canadian pediatric oncology centres. Our primary outcome was the monthly age-standardized incidence rates (ASIRs) of cancers. We evaluated level and trend changes using interventional autoregressive integrated moving average models. Secondary outcomes were the proportion of patients who were enrolled in a clinical trial, who had metastatic or advanced disease and who died within 30 days. We compared the baseline and pandemic periods using rate ratios (RRs) and 95% confidence intervals (CIs).
Results: Age-standardized incidence rates during COVID-19 quarters were 157.7, 164.6, and 148.0 per million, respectively, whereas quarterly baseline ASIRs ranged between 150.3 and 175.1 per million (incidence RR 0.93 [95% CI 0.78 to 1.12] to incidence RR 1.04 [95% CI 0.87 to 1.24]). We found no statistically significant level or slope changes between the projected and observed ASIRs for all new cancers (parameter estimate [β], level 4.98, 95% CI -15.1 to 25.04, p = 0.25), or when stratified by cancer type or by geographic area. Clinical trial enrolment rate was stable or increased during the pandemic compared with baseline (RR 1.22 [95% CI 0.70 to 2.13] to RR 1.71 [95% CI 1.01 to 2.89]). There was no difference in the proportion of patients with metastatic disease (RR 0.84 [95% CI 0.55 to 1.29] to RR 1.22 [0.84 to 1.79]), or who died within 30 days (RR 0.16 [95% CI 0.01 to 3.04] to RR 1.73 [95% CI 0.38 to 15.2]).
Interpretation: We did not observe a statistically significant change in the incidence of childhood cancer, or in the proportion of children enrolling in a clinical trial, presenting with metastatic disease or who died early during the first 9 months of the COVID-19 pandemic, which suggests that access to health care in pediatric oncology was not reduced substantially in Canada.
© 2021 CMA Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- IJzerman M, Emery J. Is a delayed cancer diagnosis a consequence of COVID-19? Victoria (AU): The University of Melbourne. Available: https://pursuit.unimelb.edu.au/articles/is-a-delayed-cancer-diagnosis-a-... (accessed 2021 Mar. 31).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical