

Global, regional and national burden of bladder cancer and its attributable risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease study 2019
- PMID: 34844997
- PMCID: PMC8634015
- DOI: 10.1136/bmjgh-2020-004128
Global, regional and national burden of bladder cancer and its attributable risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease study 2019
Abstract
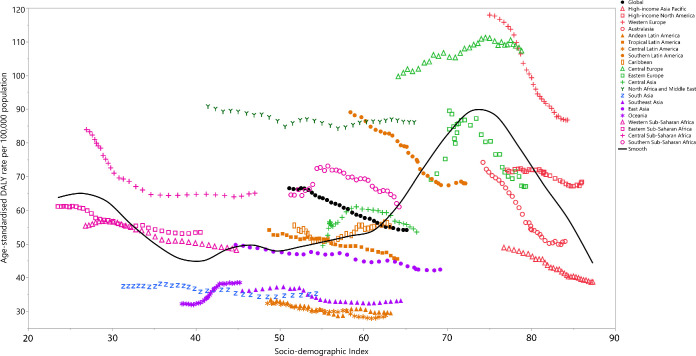
Introduction: The current study determined the level and trends associated with the incidence, death and disability rates for bladder cancer and its attributable risk factors in 204 countries and territories, from 1990 to 2019, by age, sex and sociodemographic index (SDI; a composite measure of sociodemographic factors).
Methods: Various data sources from different countries, including vital registration and cancer registries were used to generate estimates. Mortality data and incidence data transformed to mortality estimates using the mortality to incidence ratio (MIR) were used in a cause of death ensemble model to estimate mortality. Mortality estimates were divided by the MIR to produce incidence estimates. Prevalence was calculated using incidence and MIR-based survival estimates. Age-specific mortality and standardised life expectancy were used to estimate years of life lost (YLLs). Prevalence was multiplied by disability weights to estimate years lived with disability (YLDs), while disability-adjusted life years (DALYs) are the sum of the YLLs and YLDs. All estimates were presented as counts and age-standardised rates per 100 000 population.
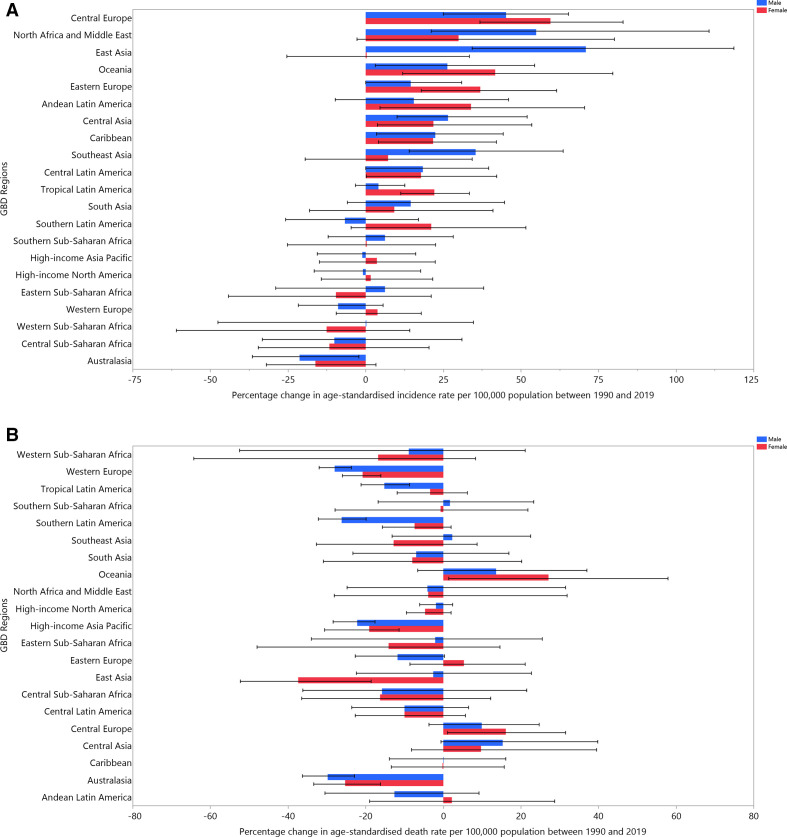
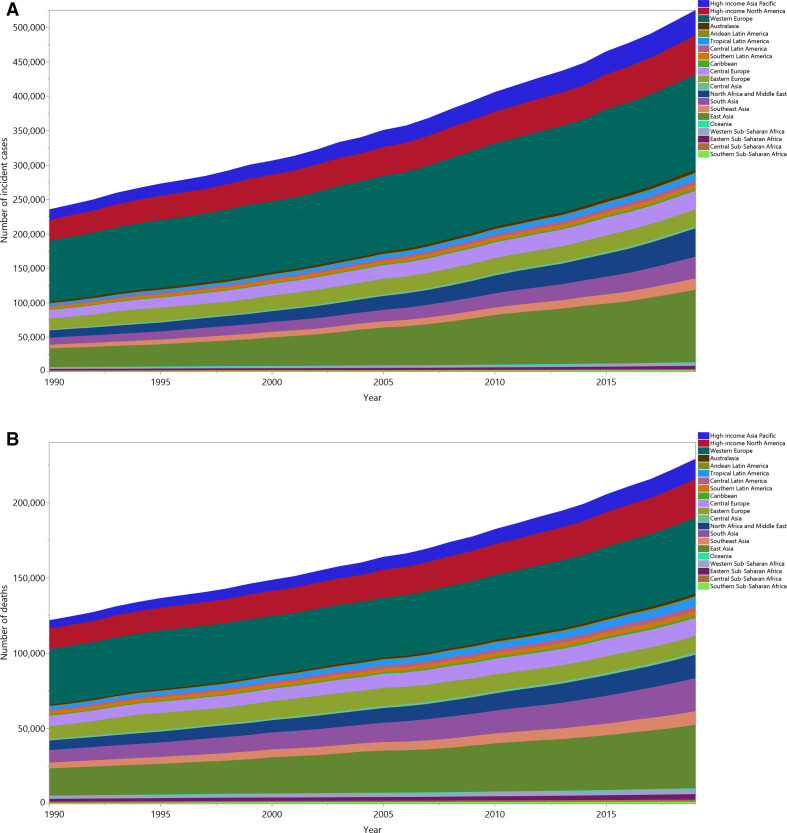
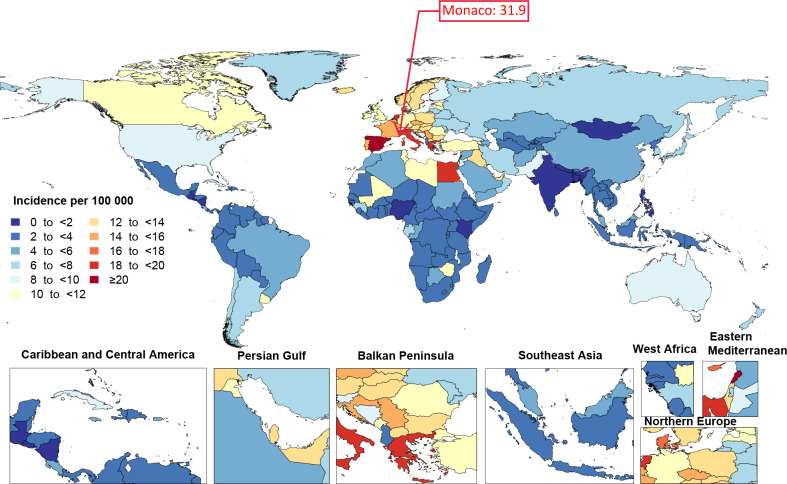
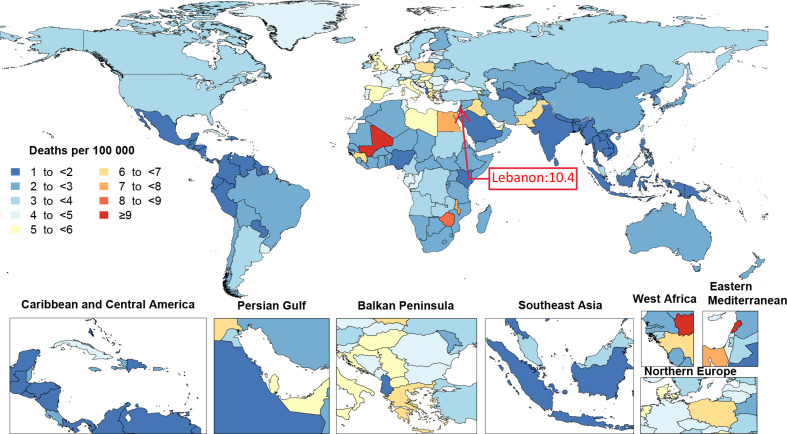
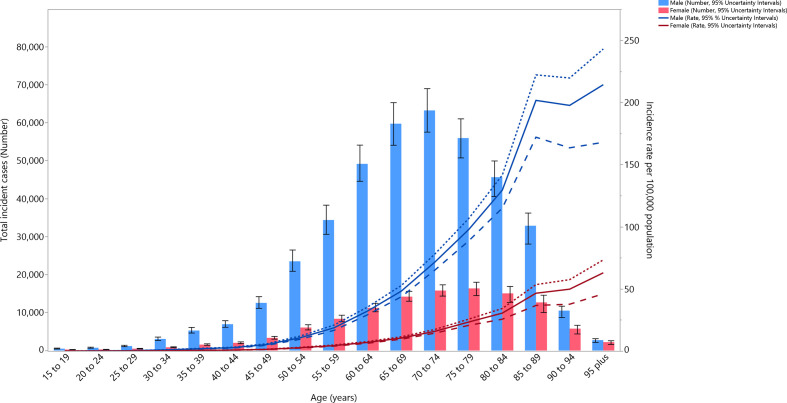
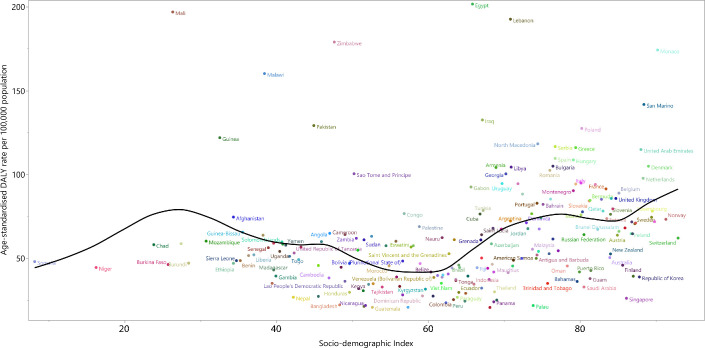
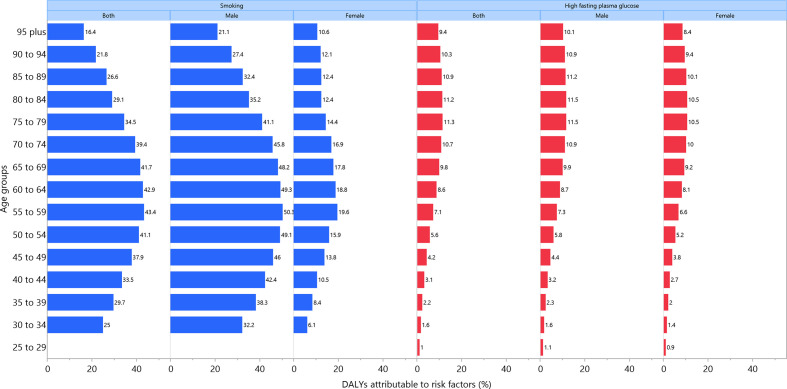
Results: Globally, there were 524 000 bladder cancer incident cases (95% uncertainty interval 476 000 to 569 000) and 229 000 bladder cancer deaths (211 000 to 243 000) in 2019. Age-standardised death rate decreased by 15.7% (8.6 to 21.0), during the period 1990-2019. Bladder cancer accounted for 4.39 million (4.09 to 4.70) DALYs in 2019, and the age-standardised DALY rate decreased significantly by 18.6% (11.2 to 24.3) during the period 1990-2019. In 2019, Monaco had the highest age-standardised incidence rate (31.9 cases (23.3 to 56.9) per 100 000), while Lebanon had the highest age-standardised death rate (10.4 (8.1 to 13.7)). Cabo Verde had the highest increase in age-standardised incidence (284.2% (214.1 to 362.8)) and death rates (190.3% (139.3 to 251.1)) between 1990 and 2019. In 2019, the global age-standardised incidence and death rates were higher among males than females, across all age groups and peaked in the 95+ age group. Globally, 36.8% (28.5 to 44.0) of bladder cancer DALYs were attributable to smoking, more so in males than females (43.7% (34.0 to 51.8) vs 15.2% (10.9 to 19.4)). In addition, 9.1% (1.9 to 19.6) of the DALYs were attributable to elevated fasting plasma glucose (FPG) (males 9.3% (1.6 to 20.9); females 8.4% (1.6 to 19.1)).
Conclusions: There was considerable variation in the burden of bladder cancer between countries during the period 1990-2019. Although there was a clear global decrease in the age-standardised death, and DALY rates, some countries experienced an increase in these rates. National policy makers should learn from these differences, and allocate resources for preventative measures, based on their country-specific estimates. In addition, smoking and elevated FPG play an important role in the burden of bladder cancer and need to be addressed with prevention programmes.
Keywords: cancer; epidemiology.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: S Safiri and A Kolahi report grants or contracts from Shahid Beheshti University of Medical Sciences, Tehran, Iran (No. 21230-4-6), outside the submitted work. G Carreras reports grants or contracts from Tuscany Region “Salute 2018” ACAB Project, Horizon 2020 EU Project TakSHS, and FP7-HEALTH EU Project ACTION as payment to their institution, all outside the submitted work. K Compton, X Dai, J Harvey, H Henrikson, and R Xu report support for the present manuscript from the Bill & Melinda Gates Foundation to the Global Burden of Disease Study through their employment at IHME. I Fillip reports payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from Avicenna Medical and Clinical Research Institute, outside the submitted work. C La Vecchia reports grants or contracts from the AIRC Foundation (Associazione Italiana per la Ricerca sul Cancro) to their institution; payment for expert testimony from Michelin, all outside the submitted work. S Mohammed reports support for the present manuscript from the Bill & Melinda Gates Foundation. A Radfar reports payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events through financial support from Avicenna Medical and Clinical Research Institute, outside the submitted work. F Sha reports support for the present manuscript from the Shenzhen Science and Technology Program as personal payments; grants or contracts from the Shenzhen Science and Technology Program as personal payments outside the submitted work. J Singh reports consulting fees from Crealta/Horizon, Medisys, Fidia, Two labs Inc, Adept Field Solutions, Clinical Care options, Clearview healthcare partners, Putnam associates, Focus forward, Navigant consulting, Spherix, MedIQ, UBM LLC, Trio Health, Medscape, WebMD, and Practice Point communications and the National Institutes of Health and the American College of Rheumatology; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Simply Speaking; support for attending meetings and/or travel from OMERACT, an international organization that develops measures for clinical trials and receives arm’s length funding from 12 pharmaceutical companies, when traveling to OMERACT meetings; participation on a Data Safety Monitoring Board or Advisory Board as a member of the FDA Arthritis Advisory Committee; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, with OMERACT as a member of the steering committee, with the Veterans Affairs Rheumatology Field Advisory Committee as a member, and with the UAB Cochrane Musculoskeletal Group Satellite Center on Network Meta-analysis as a director and editor; stock or stock options in TPT Global Tech, Vaxart pharmaceuticals, Charlotte’s Web Holdings Inc. and previously owned stock options in Amarin, Viking, and Moderna pharmaceuticals; all outside the submitted work.
Figures


References
-
- Global Burden of Disease Cancer Collaboration, Fitzmaurice C, Abate D, et al. Global, regional, and National cancer incidence, mortality, years of life lost, years lived with disability, and Disability-Adjusted life-years for 29 cancer groups, 1990 to 2017: a systematic analysis for the global burden of disease study. JAMA Oncol 2019;5:1749–68. 10.1001/jamaoncol.2019.2996 - DOI - PMC - PubMed
-
- Roth GA, Abate D, Abate KH, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the global burden of disease study 2017. The Lancet 2018;392:1736–88. 10.1016/S0140-6736(18)32203-7 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical