

Paradigm shift for defining the resectability of pancreatic cancer
- PMID: 34845115
- PMCID: PMC8639311
- DOI: 10.14701/ahbps.2021.25.4.451
Paradigm shift for defining the resectability of pancreatic cancer
Abstract
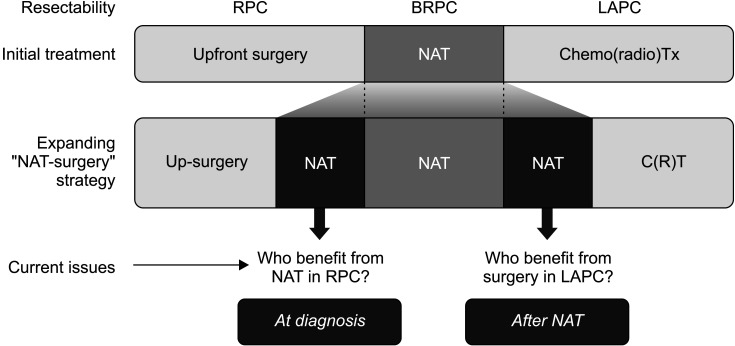
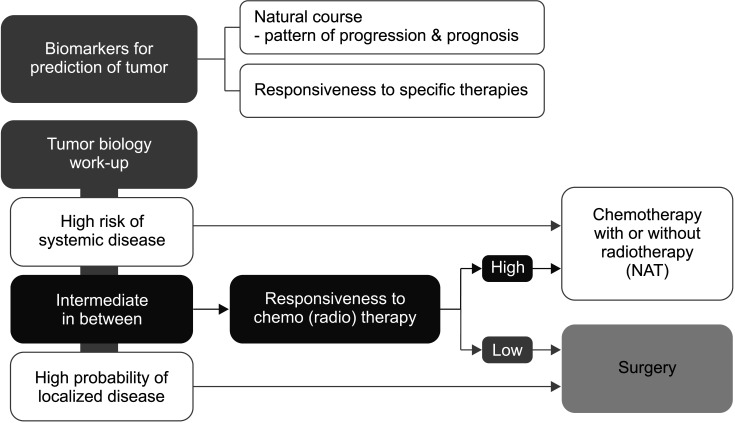
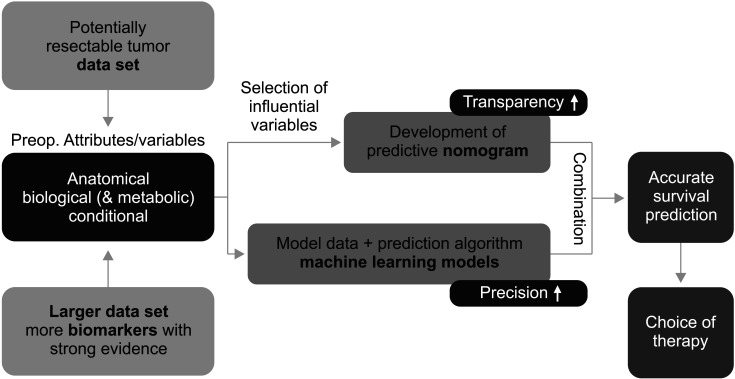
Supported by the expanding indications for neoadjuvant therapy (NAT) for advanced pancreatic cancer (PC), the concept of resectability has evolved from being mostly based on the anatomical tumor extent to considering the biological and conditional factors relevant to prognosis. Therefore, it is more reasonable to define the "criteria for surgical resection" instead of using the "(technical) resectability criteria." NAT has been used in resectable PCs (RPC) with a high risk of early systemic recurrence, as predicted by various biological or anatomical markers. Moreover, the indications for NAT followed by conversion surgery or adjuvant surgery for borderline resectable or locally advanced PC (LAPC) are gradually expanding. Therefore, it is important to define the RPC group that will benefit from NAT and the LAPC group that will benefit from post-NAT surgery. At diagnosis, population-based approaches, such as prognostic stratification and staging systems and personalized outcome-based approaches using prognostic prediction models can be used to determine the criteria for treatment options. Standardized indications for conversion surgery are needed for patients who are initially treated with NAT. In addition to imaging-based morphological criteria, biological criteria, including CA19-9, and various metabolic criteria can be used to establish predicted outcome-based criteria. Multicenter collaboration is required to develop a large database with standardized data collection for various biomarkers and response data after NAT to establish more accurate outcome prediction models to define the new resectability criteria.
Keywords: Biomarkers; Neoadjuvant therapy; Pancreatectomy; Pancreatic neoplasms; Patient selection.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- National Comprehensive Cancer Network (NCCN), author NCCN clinical practice guidelines in oncology: pancreatic adenocarcinoma, version 2 [Internet]. Plymouth Meeting: NCCN 2021. [cited 2021 Jun 5]. https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1455. Available from: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1455 .
Publication types
LinkOut - more resources
Full Text Sources