

Factors associated with hospital and intensive care admission in paediatric SARS-CoV-2 infection: a prospective nationwide observational cohort study
- PMID: 34845526
- PMCID: PMC8628837
- DOI: 10.1007/s00431-021-04276-9
Factors associated with hospital and intensive care admission in paediatric SARS-CoV-2 infection: a prospective nationwide observational cohort study
Erratum in
-
Correction to: Factors associated with hospital and intensive care admission in paediatric SARS‑CoV‑2 infection: a prospective nationwide observational cohort study.Eur J Pediatr. 2022 Mar;181(3):1257. doi: 10.1007/s00431-021-04359-7. Eur J Pediatr. 2022. PMID: 35032201 Free PMC article. No abstract available.
Abstract
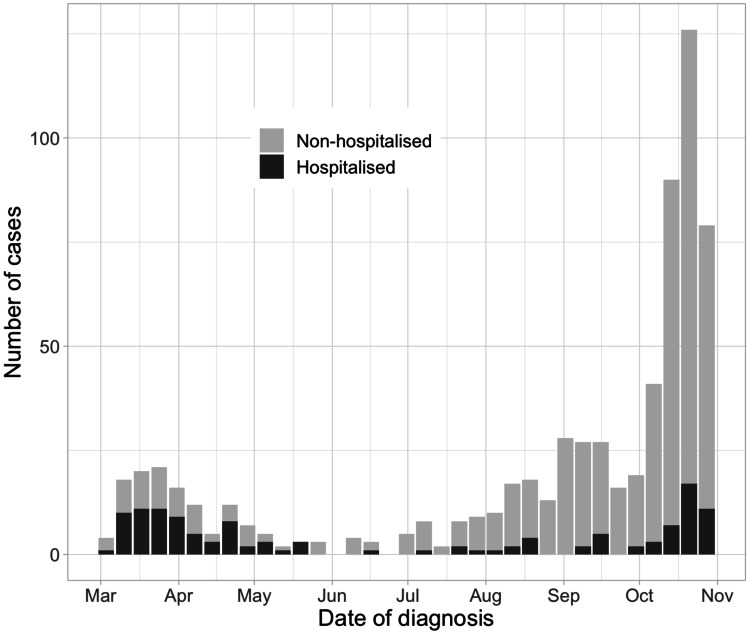
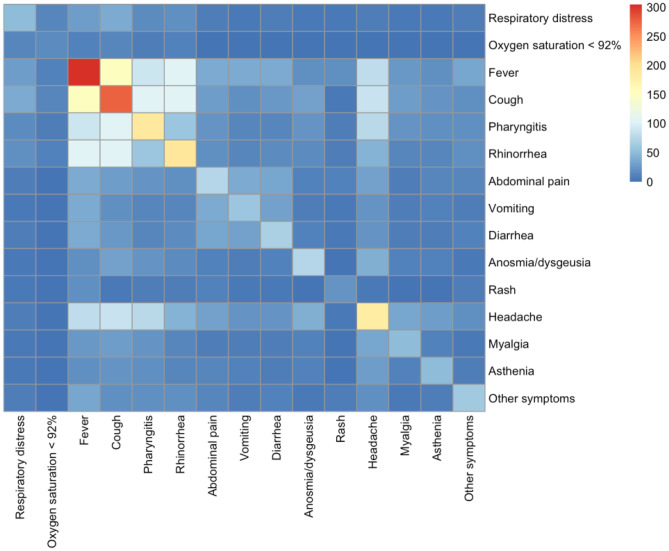
Coronavirus disease 2019 (COVID-19) is usually less severe in children compared to adults. This study describes detailed clinical characteristics, treatment and outcomes of children with COVID-19 in a non-hospitalised and hospitalised setting and quantifies factors associated with admission to hospital and intensive care unit in children with SARS-CoV-2 infection on a nationwide level. Data were collected through the Swiss Paediatric Surveillance Unit from children < 18 years with confirmed SARS-CoV-2 infection. All 33 paediatric hospitals in Switzerland reported non-hospitalised and hospitalised cases from March 1 to October 31, 2020 during both pandemic peaks. In total, 678 children were included. The median age was 12.2 years (IQR 5.0-14.6), 316 (46.6%) were female and 106 (15.6%) had comorbidities. Overall, 126 (18.6%) children were hospitalised of whom 16 (12.7%) required ICU admission. Comorbidities were the only factor associated with hospital admission in a multivariable regression analysis (odds ratio 3.23, 95%CI 1.89 to 5.50; p-value < 0.01). Children with preexisting comorbidities did not require ICU admission more often. Hospitalised children more often presented with fever (96 [76.2%] vs 209 [38.1%], p-value < 0.01) and rash (16 [12.8%] vs 6 [1.1%], p-value < 0.01). Anosmia/dysgeusia was more prevalent in non-hospitalised children (73 [13.3%] vs 3 [2.4%], p-value < 0.01). In hospitalised children, oxygen treatment was required in 34 (27.0%), inotropes in nine (7.3%) and mechanical ventilation in eight (6.3%) cases. Complications were reported in 28 (4.1%) children with cardiovascular complications being most frequent (12 [1.8%]). Three deaths were recorded.Conclusion: This study confirms that COVID-19 is mostly a mild disease in children. Fever, rash and comorbidities are associated with higher admission rates. Continuous observation is necessary to further understand paediatric COVID-19, guide therapy and evaluate the necessity for vaccination in children. What is Known: • Clinical manifestations of SARS-CoV-2 infection in children vary from asymptomatic to critical disease requiring intensive care unit admission. • Most studies are based on hospitalised children only; currently, there is limited data on non-hospitalised children. What is New: • The clinical spectrum and severity of COVID-19 is influenced by age: in children less than 2 years, fever, cough and rhinorrhoea are the most common symptoms and in adolescents, fever, cough and headache are more common. • Hospitalised children more often presented with fever and rash, while anosmia/dysgeusia is more prevalent in non-hospitalised children. • Children with pre-existing comorbidities are more frequently hospitalised but do not require ICU admission more often.
Keywords: COVID-19; Child; Clinical presentation; Epidemiology; Outcome; Transmission.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Dong Y et al (2020) Epidemiology of COVID-19 among children in China. Pediatrics 145:e20200702 - PubMed
-
- Zimmermann P, Curtis N (2020) Why is COVID-19 less severe in children ? A review of the proposed mechanisms underlying the age-related difference in severity of SARS-CoV-2 infections. 1–11. 10.1136/archdischild-2020-320338 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
