

Longitudinal Trajectories and Factors Associated With US County-Level Cardiovascular Mortality, 1980 to 2014
- PMID: 34846526
- PMCID: PMC8634057
- DOI: 10.1001/jamanetworkopen.2021.36022
Longitudinal Trajectories and Factors Associated With US County-Level Cardiovascular Mortality, 1980 to 2014
Abstract
Importance: Cardiovascular (CV) mortality has declined for more than 3 decades in the US. However, differences in declines among residents at a US county level are not well characterized.
Objective: To identify unique county-level trajectories of CV mortality in the US during a 35-year study period and explore county-level factors that are associated with CV mortality trajectories.
Design, setting, and participants: This longitudinal cross-sectional analysis of CV mortality trends used data from 3133 US counties from 1980 to 2014. County-level demographic, socioeconomic, environmental, and health-related risk factors were compiled. Data were analyzed from December 2019 to September 2021.
Exposures: County-level characteristics, collected from 5 county-level data sets.
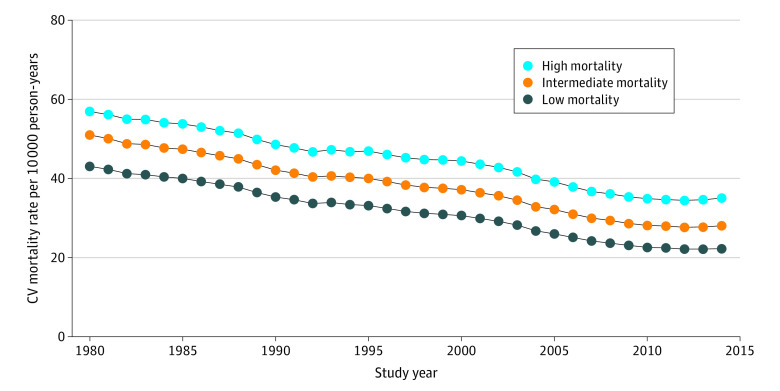
Main outcomes and measures: Cardiovascular mortality data were obtained for 3133 US counties from 1980 to 2014 using age-standardized county-level mortality rates from the Global Burden of Disease study. The longitudinal K-means approach was used to identify 3 distinct clusters based on underlying mortality trajectory. Multinomial logistic regression models were constructed to evaluate associations between county characteristics and cluster membership.
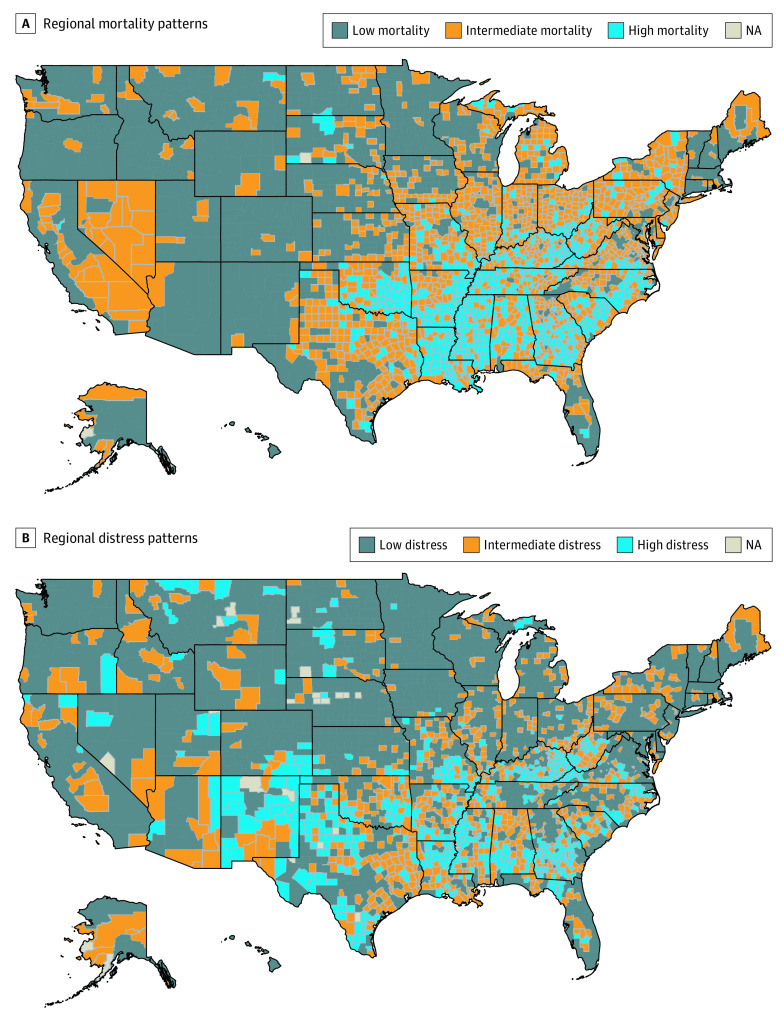
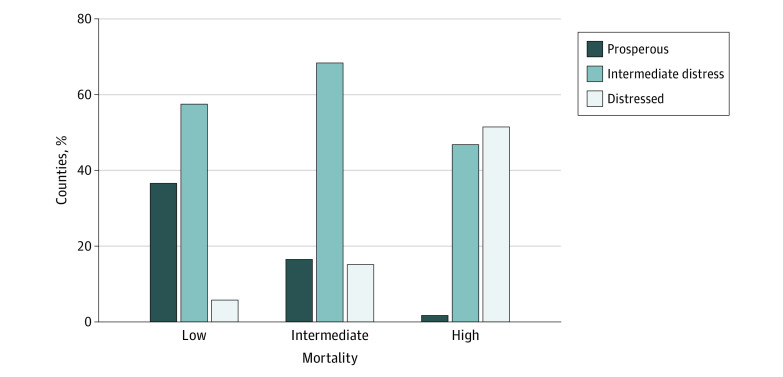
Results: Among 3133 US counties (median, 49.5% [IQR, 48.9%-50.5%] men; 30.7% [IQR, 27.1%-34.4%] older than 55 years; 9.9% [IQR, 4.5%-22.7%] racial minority group [individuals self-identifying as Black or African American, American Indian or Alaska Native, Asian, Native Hawaiian, Pacific Islander, other, or multiple races/ethnicities]), CV mortality declined by 45.5% overall and by 38.4% in high-mortality strata (694 counties), by 45.0% in intermediate-mortality strata (1382 counties), and by 48.3% in low-mortality strata (1057 counties). Counties with the highest mortality in 1980 continued to demonstrate the highest mortality in 2014. Trajectory groups were regionally distributed, with high-mortality trajectory counties focused in the South and in portions of Appalachia. Low- vs high-mortality groups varied significantly in demographic (racial minority group proportion, 7.6% [IQR, 4.1%-14.5%]) vs 23.9% [IQR, 6.5%-40.8%]) and socioeconomic characteristics such as high-school education (9.4% [IQR, 7.3%-12.6%] vs 20.1% [IQR, 16.1%-23.2%]), poverty rates (11.4% [IQR, 8.8%-14.6%] vs 20.6% [IQR, 17.1%-24.4%]), and violent crime rates (161.5 [IQR, 89.0-262.4] vs 272.8 [IQR, 155.3-431.3] per 100 000 population). In multinomial logistic regression, a model incorporating demographic, socioeconomic, environmental, and health characteristics accounted for 60% of the variance in the CV mortality trajectory (R2 = 0.60). Sociodemographic factors such as racial minority group proportion (odds ratio [OR], 1.70 [95% CI, 1.35-2.14]) and educational attainment (OR, 6.17 [95% CI, 4.55-8.36]) and health behaviors such as smoking (OR for high vs low, 2.04 [95% CI, 1.58-2.64]) and physical inactivity (OR, 3.74 [95% CI, 2.83-4.93]) were associated with the high-mortality trajectory.
Conclusions and relevance: Cardiovascular mortality declined in all subgroups during the 35-year study period; however, disparities remained unchanged during that time. Disparate trajectories were associated with social and behavioral risks. Health policy efforts across multiple domains, including structural and public health targets, may be needed to reduce existing county-level cardiovascular mortality disparities.
Conflict of interest statement
Figures
References
-
- Havranek EP, Mujahid MS, Barr DA, et al. ; American Heart Association Council on Quality of Care and Outcomes Research, Council on Epidemiology and Prevention, Council on Cardiovascular and Stroke Nursing, Council on Lifestyle and Cardiometabolic Health, and Stroke Council . Social determinants of risk and outcomes for cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2015;132(9):873-898. doi: 10.1161/CIR.0000000000000228 - DOI - PubMed
