

Cognitive behavioral therapy for irritable bowel syndrome induces bidirectional alterations in the brain-gut-microbiome axis associated with gastrointestinal symptom improvement
- PMID: 34847963
- PMCID: PMC8630837
- DOI: 10.1186/s40168-021-01188-6
Cognitive behavioral therapy for irritable bowel syndrome induces bidirectional alterations in the brain-gut-microbiome axis associated with gastrointestinal symptom improvement
Abstract
Background: There is growing recognition that bidirectional signaling between the digestive tract and the brain contributes to irritable bowel syndrome (IBS). We recently showed in a large randomized controlled trial that cognitive behavioral therapy (CBT) reduces IBS symptom severity. This study investigated whether baseline brain and gut microbiome parameters predict CBT response and whether response is associated with changes in the brain-gut-microbiome (BGM) axis.
Methods: Eighty-four Rome III-diagnosed IBS patients receiving CBT were drawn from the Irritable Bowel Syndrome Outcome Study (IBSOS; ClinicalTrials.gov NCT00738920) for multimodal brain imaging and psychological assessments at baseline and after study completion. Fecal samples were collected at baseline and post-treatment from 34 CBT recipients for 16S rRNA gene sequencing, untargeted metabolomics, and measurement of short-chain fatty acids. Clinical measures, brain functional connectivity and microstructure, and microbiome features associated with CBT response were identified by multivariate linear and negative binomial models.
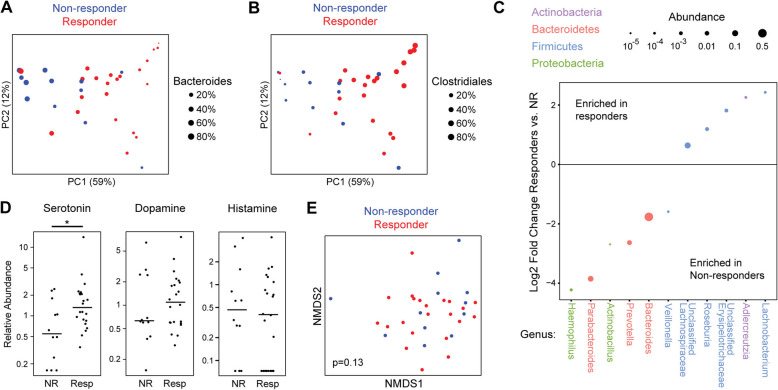
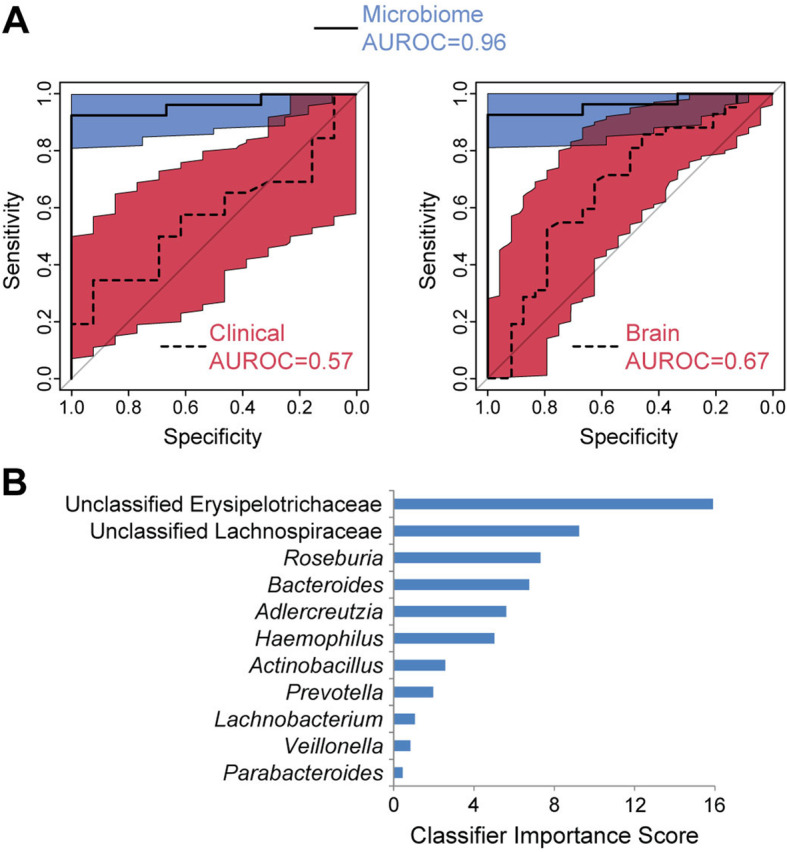
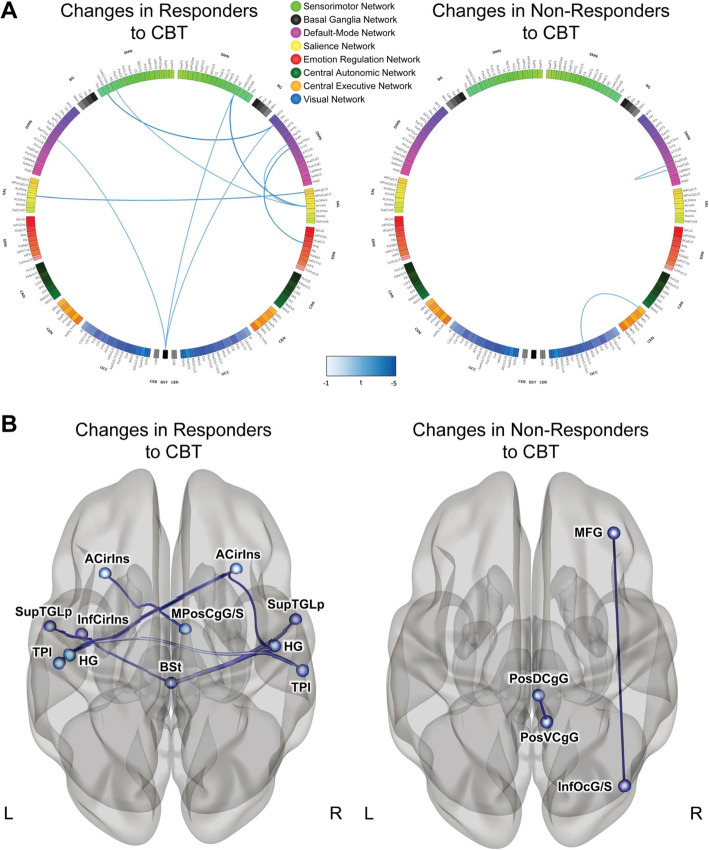
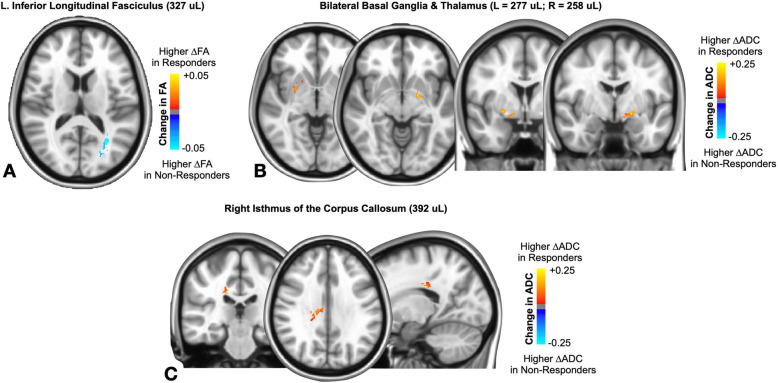
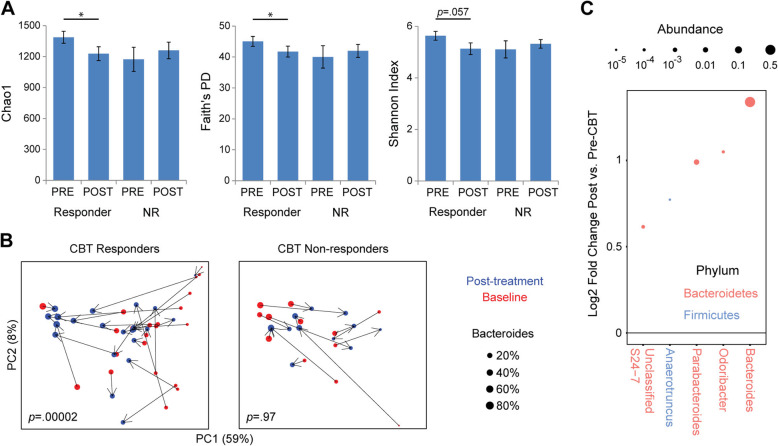
Results: At baseline, CBT responders had increased fecal serotonin levels, and increased Clostridiales and decreased Bacteroides compared to non-responders. A random forests classifier containing 11 microbial genera predicted CBT response with high accuracy (AUROC 0.96). Following treatment, CBT responders demonstrated reduced functional connectivity in regions of the sensorimotor, brainstem, salience, and default mode networks and changes in white matter in the basal ganglia and other structures. Brain changes correlated with microbiome shifts including Bacteroides expansion in responders.
Conclusions: Pre-treatment intestinal microbiota and serotonin levels were associated with CBT response, suggesting that peripheral signals from the microbiota can modulate central processes affected by CBT that generate abdominal symptoms in IBS. CBT response is characterized by co-correlated shifts in brain networks and gut microbiome that may reflect top-down effects of the brain on the microbiome during CBT. Video abstract.
Keywords: Biomarkers; Brain-gut-microbiome axis; Cognitive behavioral therapy; Irritable bowel syndrome; Neuroimaging; Outcome prediction.
© 2021. The Author(s).
Conflict of interest statement
EAM is a scientific advisory board member of Danone, Axial Biotherapeutics, Viome, Amare, Mahana Therapeutics, Pendulum, Bloom Biosciences, APC Microbiome Ireland. BME is an advisor for Hoffman La-Roche; Siemens; Nativis; Medicenna; MedQIA; Bristol Meyers Squibb; Imaging Endpoints; VBL; and Agios Pharmaceuticals. BME is a Paid Consultant for Nativis; MedQIA; Siemens; Hoffman La-Roche; Imaging Endpoints; Medicenna; and Agios. BME received grant funding from Siemens, Agios, and Janssen. JPJ, AG, RRB, JB, KG, KT, VL, RF, GG, JSL, BDN, and JML do not have any disclosures.
Figures
References
-
- American College of Gastroenterology Task Force on Irritable Bowel S, Brandt LJ, Chey WD, Foxx-Orenstein AE, Schiller LR, Schoenfeld PS, Spiegel BM, Talley NJ, Quigley EM: An evidence-based position statement on the management of irritable bowel syndrome. Am J Gastroenterol 2009, 104 Suppl 1:S1-35. - PubMed
-
- Spiegel B, Camilleri M, Bolus R, Andresen V, Chey WD, Fehnel S, Mangel A, Talley NJ, Whitehead WE: Psychometric evaluation of patient-reported outcomes in irritable bowel syndrome randomized controlled trials: a Rome Foundation report. Gastroenterology 2009, 137(6):1944-1953 e1941-1943. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
