

The effects of nebulized ketamine and intravenous magnesium sulfate on corticosteroid resistant asthma exacerbation; a randomized clinical trial
- PMID: 34847965
- PMCID: PMC8630847
- DOI: 10.1186/s40733-021-00081-1
The effects of nebulized ketamine and intravenous magnesium sulfate on corticosteroid resistant asthma exacerbation; a randomized clinical trial
Abstract
Background and aims: Asthma exacerbation is defined as an acute attack of shortness of breath with more than 25% decrease in morning peak flow compared to the baseline on 2 consecutive days, which requires immediate standard therapy. The majority of asthmatic patients are considered to be steroid-sensitive; however, corticosteroid-resistant asthma is a subset of asthma with poor response to corticosteroids and is responsible for frequent hospital admissions. In this study we aimed to compare the effects of two enhancing strategies, the nebulized ketamine and IV magnesium sulfate, in treatment of severe steroid resistant asthma.
Materials and methods: This double-blind randomized clinical trial was conducted on patients who presented to a referral clinic in Alborz, Iran. Using random allocation, patients were divided into two groups. The first group was treated with nebulized ketamine and the second group was treated with intravenous magnesium sulfate. Peak expiratory flow rates were assessed before the intervention, 30 and 60 min after the intervention and compared with the aid of SPSS software.
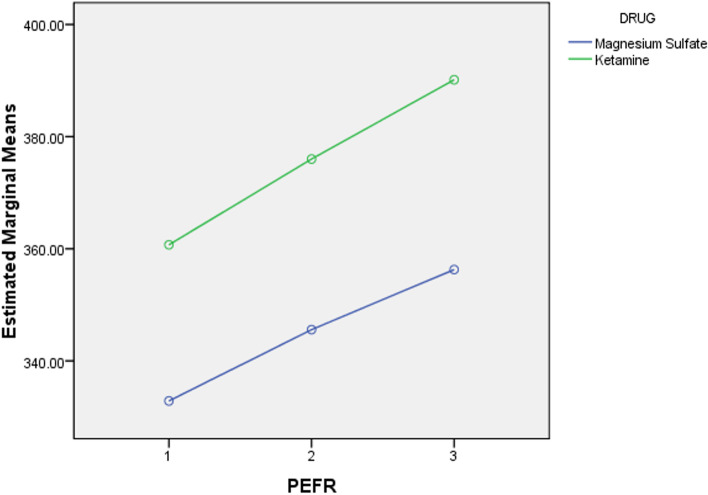
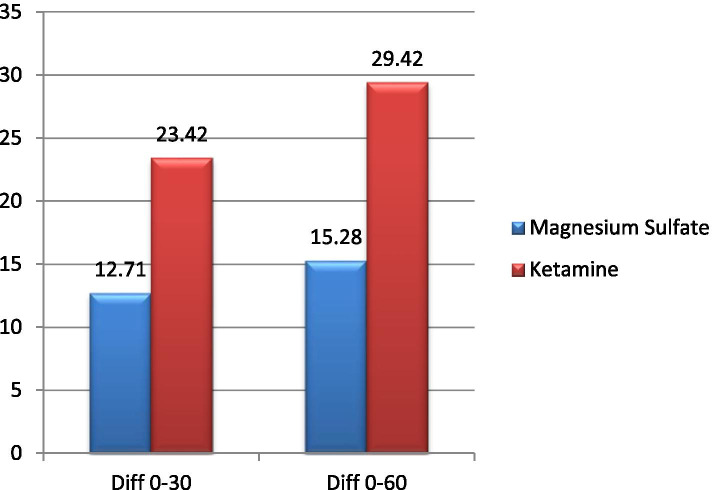
Results: The Peak expiratory flow rates before the intervention, 30 min and 60 min after the intervention was statistically significantly different in both ketamine and magnesium sulfate groups. Peak expiratory flow rates change between 0 and 60 min were 29.4 and 15.2% in the ketamine and magnesium sulfate group respectively. Although the ketamine group showed much higher increase in mean PEFR compared to the MgSO4 groups, there was no statistically significant difference across both groups.
Conclusion: Our study concluded that combined with standard therapy, both ketamine and IV magnesium sulfate are effective agents in the improvement of PEFR in patients with acute severe asthma that failed to respond to traditional therapies. However, there were no statistically significant difference between the two groups.
Keywords: Asthma; Ketamine; Magnesium sulfate; Peak expiratory flow rate.
© 2021. The Author(s).
Conflict of interest statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Figures
References
LinkOut - more resources
Full Text Sources
