

Forced-air warming and continuous core temperature monitoring with zero-heat-flux thermometry during cesarean section: a retrospective observational cohort study
- PMID: 34848308
- PMCID: PMC9373610
- DOI: 10.1016/j.bjane.2021.10.007
Forced-air warming and continuous core temperature monitoring with zero-heat-flux thermometry during cesarean section: a retrospective observational cohort study
Abstract
Background: Over 30% of parturients undergoing spinal anesthesia for cesarean section become intraoperatively hypothermic. This study assessed the magnitude of hypothermic insult in parturients and newborns using continuous, high-resolution thermometry and evaluated the efficiency of intraoperative forced-air warming for prevention of hypothermia.
Methods: One hundred and eleven parturients admitted for elective or emergency cesarean section under spinal anesthesia with newborn bonding over a 5-month period were included in this retrospective observational cohort study. Patients were divided into two groups: the passive insulation group, who received no active warming, and the active warming group, who received convective warming through an underbody blanket. Core body temperature was continuously monitored by zero-heat-flux thermometry and automatically recorded by data-loggers. The primary outcome was the incidence of hypothermia in the operating and recovery room. Neonatal outcomes were also analyzed.
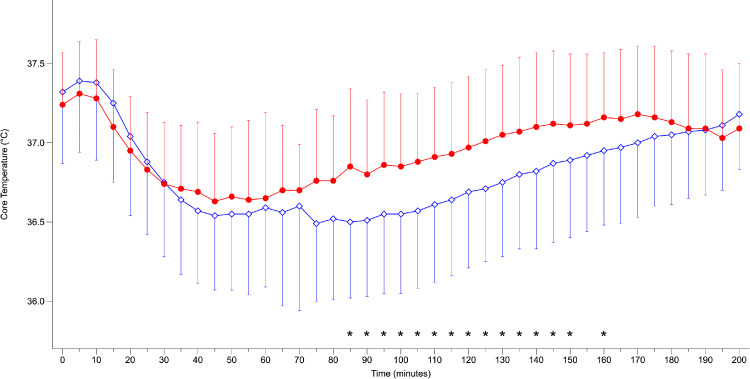
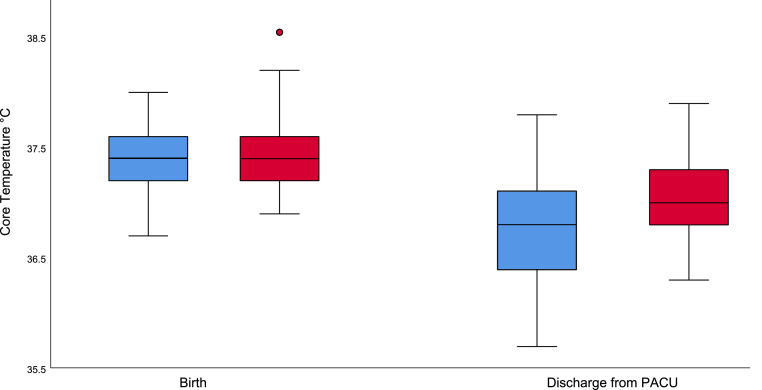
Results: The patients in the passive insulation group had significantly lower temperatures in the operating room compared to the actively warmed group (36.4°C vs. 36.6°C, p = 0.005), including temperature at skin closure (36.5°C vs. 36.7°C, p = 0.017). The temperature of the newborns after discharge from the postanesthetic care unit was lower in the passive insulation group (36.7°C vs. 37.0°C, p = 0.002); thirteen (15%) of the newborns were hypothermic, compared to three (4%) in the active warming group (p < 0.01).
Conclusion: Forced-air warming decreases perioperative hypothermia in parturients undergoing cesarean section but does not entirely prevent hypothermia in newborns while bonding. Therefore, it can be effectively used for cesarean section, but special attention should be given to neonates.
Keywords: Cesarean section; Core temperature; Hypothermia; Newborn bonding; Zero-heat-flux.
Copyright © 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. All rights reserved.
Conflict of interest statement
Conflicts of interest LM has received payments for lectures from 3 M. JH has received payments for lectures from 3 M, The Surgical Company and Abbvie. The other authors have no conflicts of interest to declare. The Bair Hugger(TM) temperature sensors and warming blankets were provided by 3M(TM) Deutschland GmbH, Neuss Germany; the company has played no role in this research nor in the decision to submit the article for publication.
Figures


References
-
- Juang J, Gabriel RA, Dutton RP, et al. Choice of Anesthesia for Cesarean Delivery: An Analysis of the National Anesthesia Clinical Outcomes Registry. Anesth Analg. 2017;124:1914–1917. - PubMed
-
- Clinical-Practice-Guideline. The management of inadvertent perioperative hypothermia in adults. The National Collaborating Centre for Nursing and Supportive Care commissioned by National Institute for Health and Clinical Excellence (NICE): Updated 14 December 2016. Available at: www.nice.org.uk/guidance/cg65. [accessed 08 January 2021].
-
- Melling AC, Ali B, Scott EM, et al. Effects of preoperative warming on the incidence of wound infection after clean surgery: a randomised controlled trial. Lancet. 2001;358:876–880. - PubMed
-
- Schmied H, Kurz A, Sessler DI, et al. Mild hypothermia increases blood loss and transfusion requirements during total hip arthroplasty. Lancet. 1996;347:289–292. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
