

Tranexamic acid for intracerebral haemorrhage within 2 hours of onset: protocol of a phase II randomised placebo-controlled double-blind multicentre trial
- PMID: 34848566
- PMCID: PMC9067256
- DOI: 10.1136/svn-2021-001070
Tranexamic acid for intracerebral haemorrhage within 2 hours of onset: protocol of a phase II randomised placebo-controlled double-blind multicentre trial
Abstract
Rationale: Haematoma growth is common early after intracerebral haemorrhage (ICH), and is a key determinant of outcome. Tranexamic acid, a widely available antifibrinolytic agent with an excellent safety profile, may reduce haematoma growth.
Methods and design: Stopping intracerebral haemorrhage with tranexamic acid for hyperacute onset presentation including mobile stroke units (STOP-MSU) is a phase II double-blind, randomised, placebo-controlled, multicentre, international investigator-led clinical trial, conducted within the estimand statistical framework.
Hypothesis: In patients with spontaneous ICH, treatment with tranexamic acid within 2 hours of onset will reduce haematoma expansion compared with placebo.
Sample size estimates: A sample size of 180 patients (90 in each arm) would be required to detect an absolute difference in the primary outcome of 20% (placebo 39% vs treatment 19%) under a two-tailed significance level of 0.05. An adaptive sample size re-estimation based on the outcomes of 144 patients will allow a possible increase to a prespecified maximum of 326 patients.
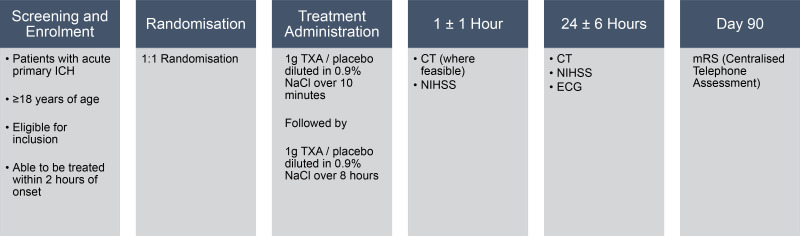
Intervention: Participants will receive 1 g intravenous tranexamic acid over 10 min, followed by 1 g intravenous tranexamic acid over 8 hours; or matching placebo.
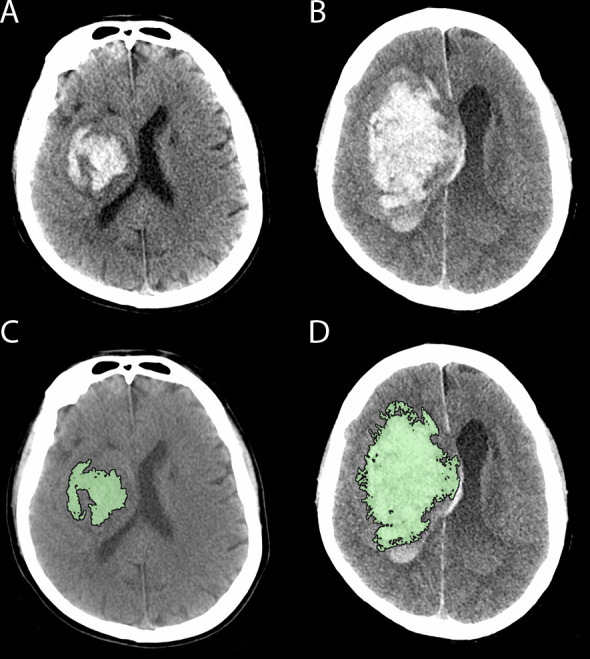
Primary efficacy measure: The primary efficacy measure is the proportion of patients with haematoma growth by 24±6 hours, defined as either ≥33% relative increase or ≥6 mL absolute increase in haematoma volume between baseline and follow-up CT scan.
Discussion: We describe the rationale and protocol of STOP-MSU, a phase II trial of tranexamic acid in patients with ICH within 2 hours from onset, based in participating mobile stroke units and emergency departments.
Keywords: CT; hemorrhage; stroke.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: Henry Zhao has received grant funding from the Medical Research Future Fund (Commonwealth Government of Australia). Leonid Churilov is co-chairperson of the Australasian Stroke Trials Network (unpaid). Andrew Cheung has received honoraria for lectures/presentations from Medtronic and Stryker and support for attending meetings and/or travel from Stryker. Rohan Grimley is a member of the Clinical Council, Stroke Foundation (Australia). Chung Hsu has received grants from the Ministry of Health and Welfare in Taiwan. Peter Mitchell has received institutional research grants from Stryker and Medtronic, travel support for attendance of international conferences and honoraria for speaking at symposia from Stryker, and is an executive member and immediate past president of the Australian and New Zealand Society of Neuroradiology (ANZSNR).
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources