

Plasma metabolomics in the perioperative period of defect repair in patients with pulmonary arterial hypertension associated with congenital heart disease
- PMID: 34848852
- PMCID: PMC9253009
- DOI: 10.1038/s41401-021-00804-3
Plasma metabolomics in the perioperative period of defect repair in patients with pulmonary arterial hypertension associated with congenital heart disease
Abstract
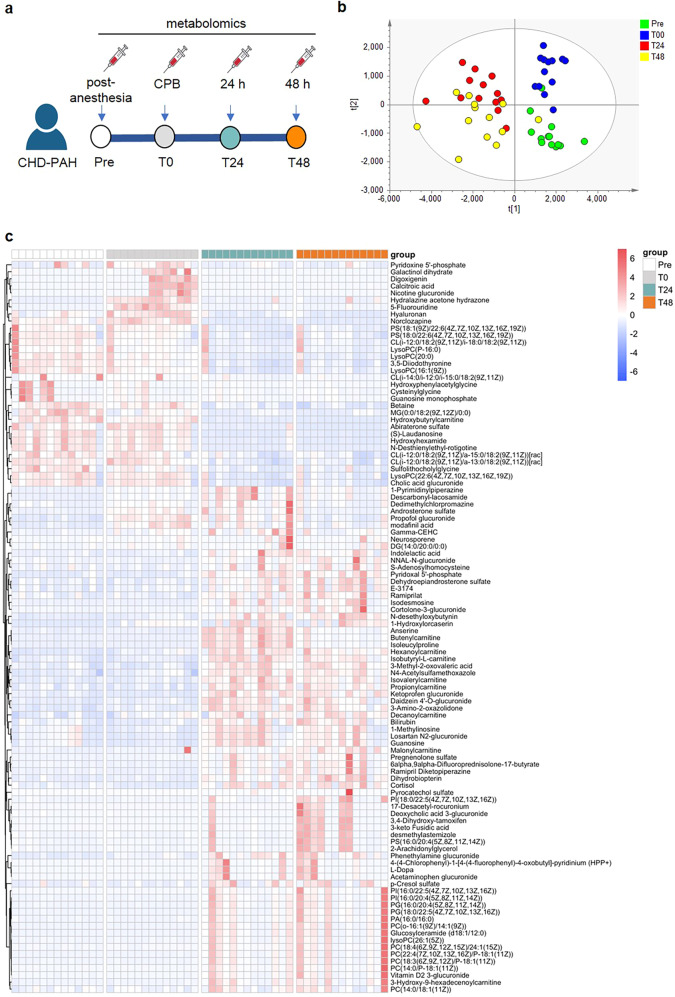
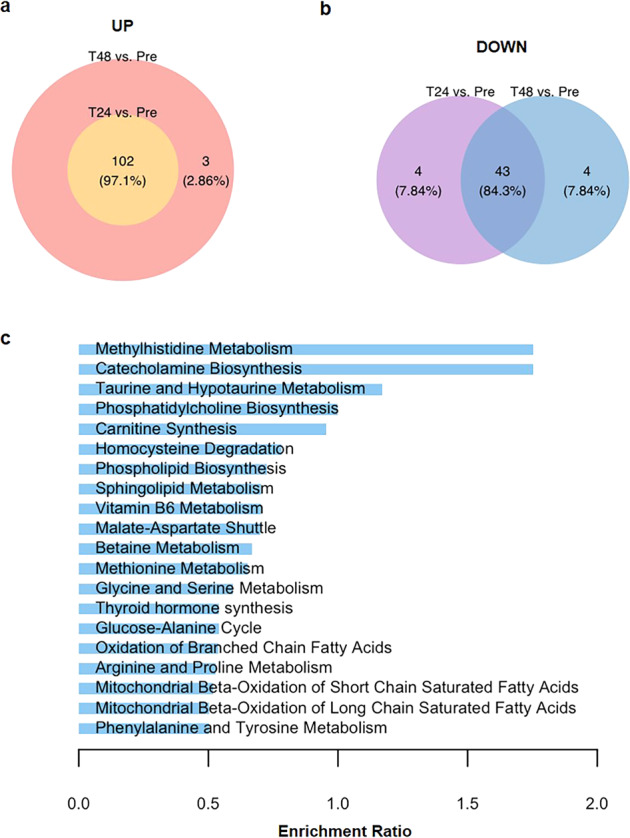
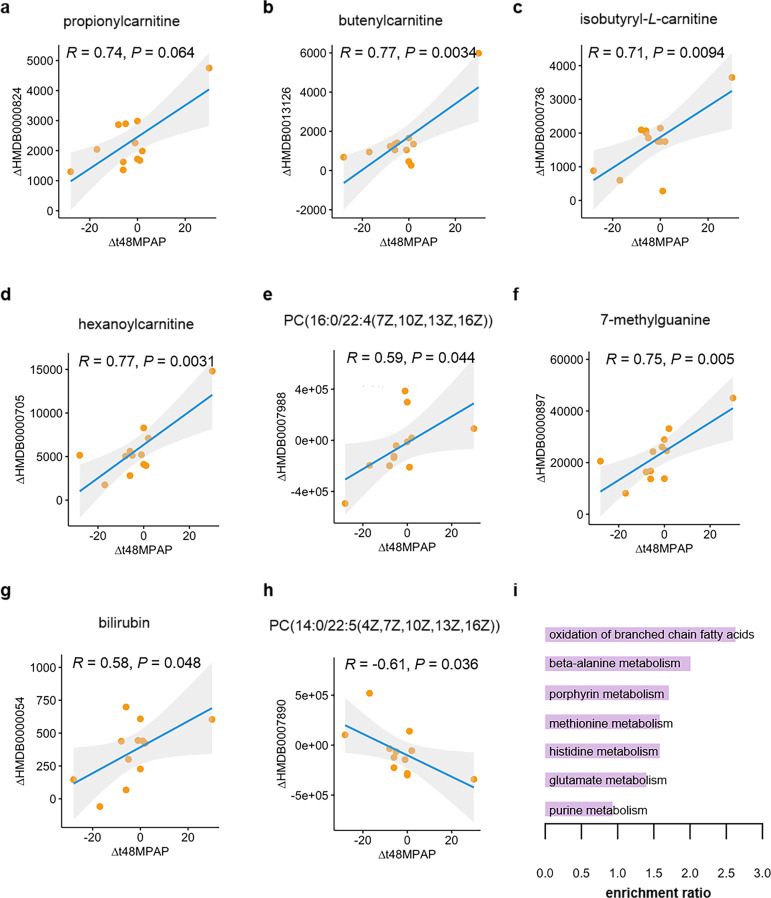
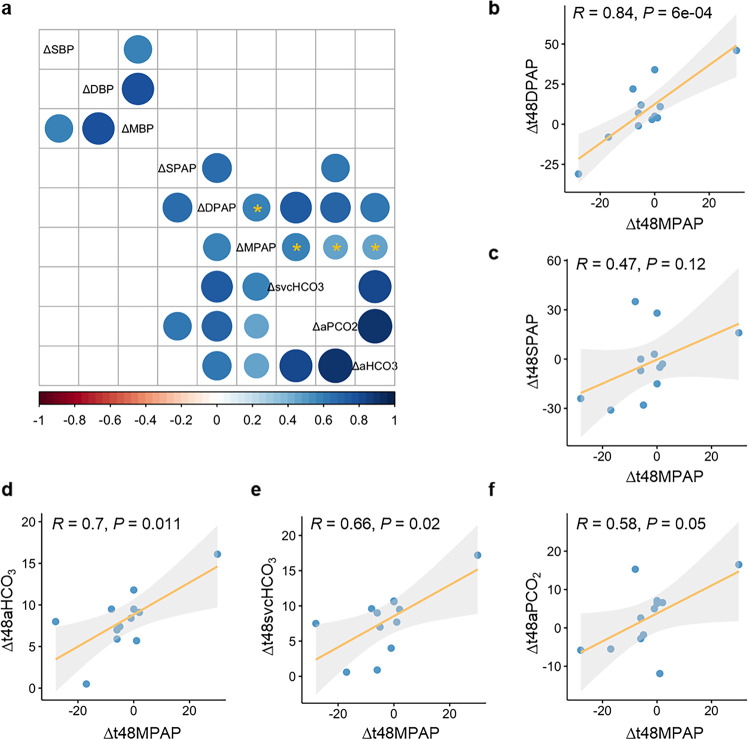
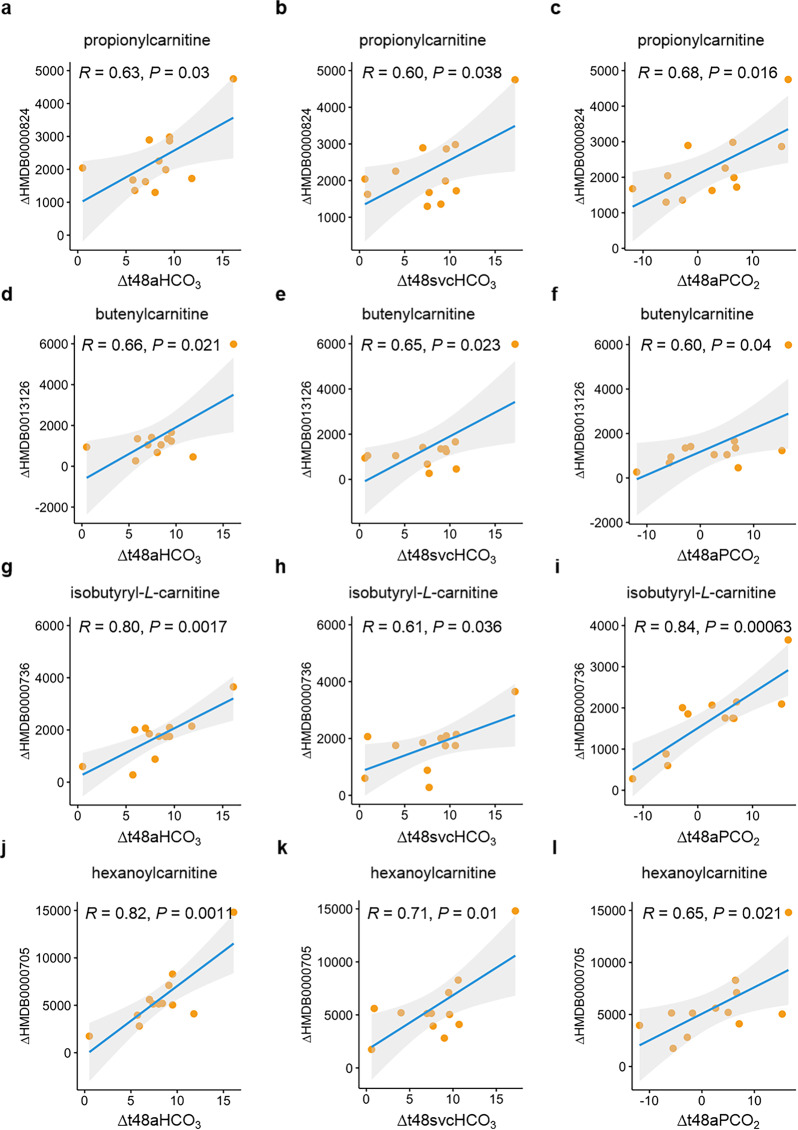
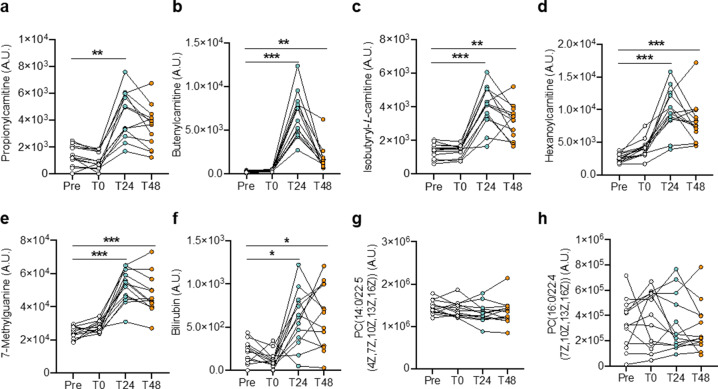
The quality of life and survival rates of patients with pulmonary arterial hypertension associated with congenital heart disease (CHD-PAH) have been greatly improved by defect-repair surgery and personalized treatments. However, those who survive surgery may remain at risk of persistent PAH, the prognosis may be considerably worse than those unoperated. Dynamic monitoring of clinical measures during the perioperative period of shunt correction is therefore indispensable and of great value. In this study, we explored the plasma-metabolite profiling in 13 patients with CHD-PAH during the perioperative period of defect repair. Plasma was harvested at four time points: prior to cardiopulmonary bypass (CPB) after anesthesia (Pre), immediately after CPB (T0), 24 h (T24), and 48 h (T48) after defect repair. Untargeted metabolomics strategy based on UPLC Q-TOF MS was used to detect the metabolites. A total of 193 distinguishing metabolites were determined at different time points, enriched in pathways such as oxidation of branched-chain fatty acids. We found that 17 metabolite alterations were significantly correlated with the reduction in mean pulmonary arterial pressure (MPAP) at T48 versus Pre. Gradients in diastolic pulmonary arterial pressure (DPAP), bicarbonate in radial artery (aHCO3), bicarbonate in superior vena cava (svcHCO3), and the partial pressure of dissolved CO2 gas in radial artery (aPCO2) were positively correlated with MPAP gradient. Notably, these clinical-measure gradients were correlated with alterations in shunt-correction-associated metabolites. In total, 12 out of 17 identified metabolites in response to defect repair were increased at both T24 and T48 (all P < 0.05, except propionylcarnitine with P < 0.05 at T24). In contrast, galactinol dihydrate, guanosine monophosphate, and hydroxyphenylacetylglycine tended to decline at T24 and T48 (only galactinol dihydrate with P < 0.05 at T48). In conclusion, 17 metabolites that respond to shunt correction could be used as suitable noninvasive markers, and clinical measures, including DPAP, aHCO3, svcHCO3, and aPCO2, would be of great value in disease monitoring and evaluating future therapeutic interventions.
Keywords: congenital heart disease; defect-repair surgery; metabolites; metabolomics; perioperative period; pulmonary arterial hypertension; pulmonary circulation.
© 2021. The Author(s), under exclusive licence to CPS and SIMM.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Galie N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT) Eur Heart J. 2016;37:67–119. doi: 10.1093/eurheartj/ehv317. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
