

Isolated Sixth Nerve Palsy as a First Presentation of Nasopharyngeal Carcinoma: A Case Series
- PMID: 34849037
- PMCID: PMC8627281
- DOI: 10.2147/IMCRJ.S334476
Isolated Sixth Nerve Palsy as a First Presentation of Nasopharyngeal Carcinoma: A Case Series
Abstract
Purpose: To describe isolated sixth nerve palsy as an uncommon presentation of nasopharyngeal carcinoma (NPC).
Patients and methods: We analyzed the demographics, clinical presentation, neuroimaging findings, and pathological examination results of the nasopharyngeal masses of patients diagnosed with isolated sixth nerve palsy due to NPC.
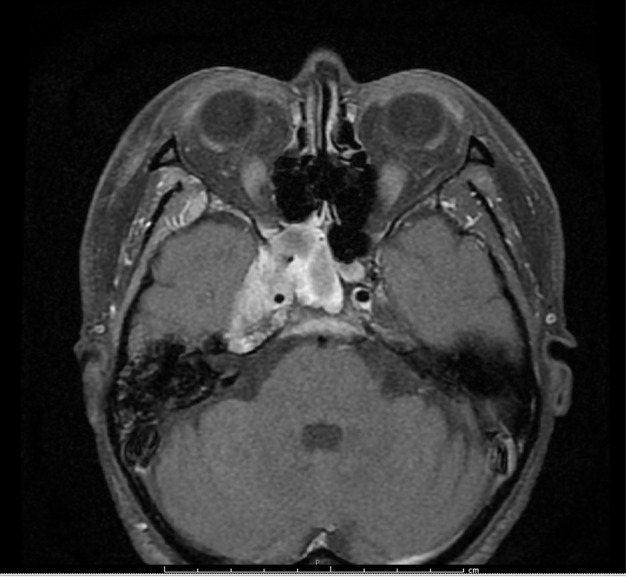
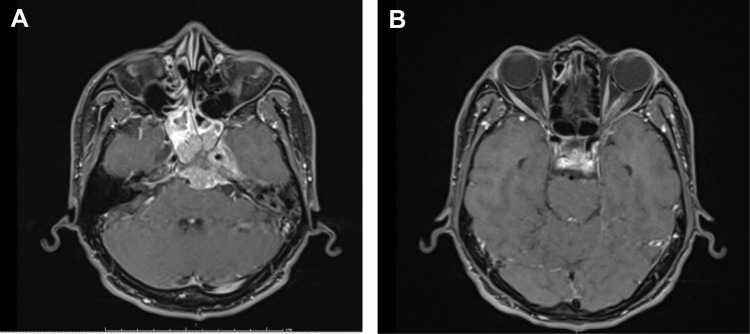
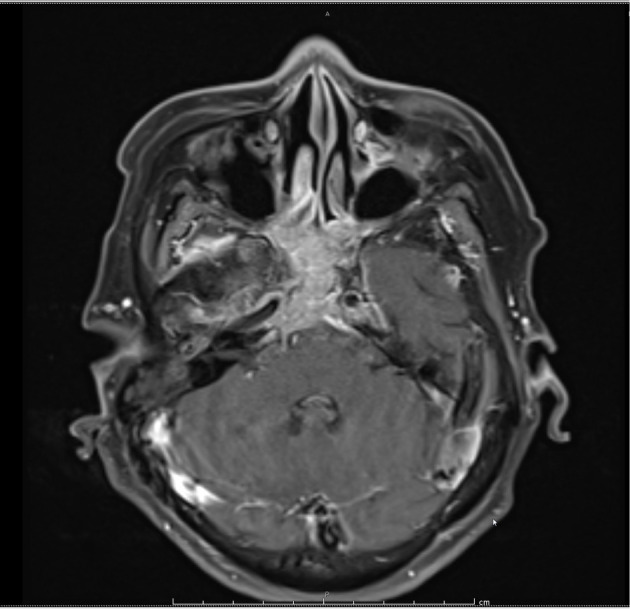
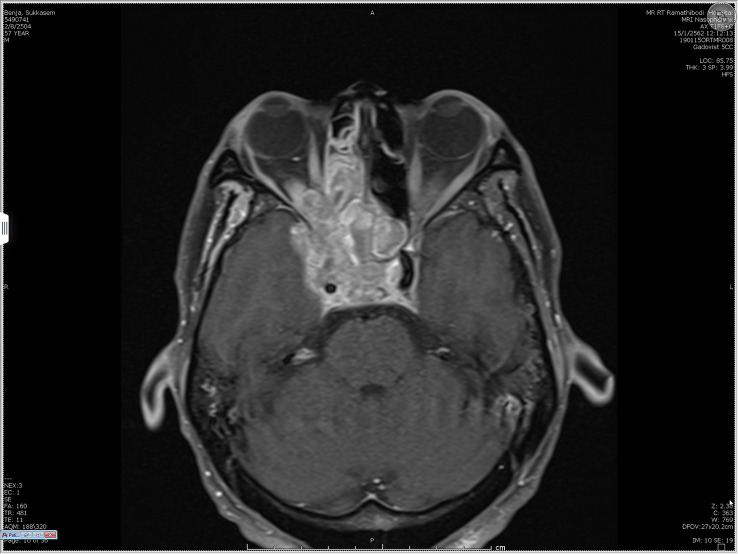
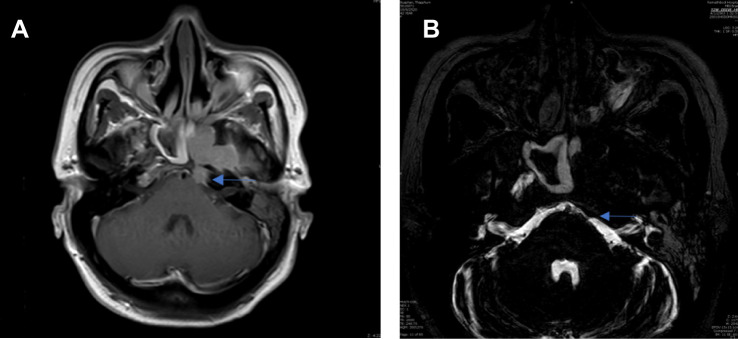
Results: Isolated sixth nerve palsy as the first presenting sign of NPC was diagnosed in five patients. Two patients were aged <50 years and three were aged >50 years, and one of these three older patients had vascular risk factors. Most of the patients in our case study had an uncommon presentation of isolated sixth nerve palsy with diplopia, followed by typical NPC signs such as a neck lump (two patients), nasal obstruction (two patients), tinnitus (two patients), hearing loss (one patient), and epistaxis (one patient). Pathological examination revealed non-keratinizing NPC in all cases. Neuroimaging showed that the sites of tumor invasion were the clivus, Dorello's canal, and cavernous sinus, which explained the sixth nerve palsy. One patient whose NPC had progressed to the orbital apex later developed other cranial nerve palsies. Three patients underwent concurrent chemoradiotherapy (CCRT), and one patient underwent CCRT with adjuvant chemotherapy. The last patient was unfortunately lost to follow-up. The symptoms of four patients who underwent treatment improved.
Conclusion: Isolated sixth nerve palsy can be the first presentation of NPC, especially in patients aged <50 years old without microvascular risk factors or even in patients aged >50 years old with microvascular risk factors. This case study emphasizes that a thorough clinical history and careful physical and neuroimaging examinations might be necessary to rule out life-threatening conditions in patients with isolated sixth nerve palsy.
Keywords: abducens nerve; diplopia; neck mass; paralytic strabismus.
© 2021 Lekskul et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Cause of acquired onset of diplopia due to isolated third, fourth, and sixth cranial nerve palsies in patients aged 20 to 50 years in Korea: A high resolution magnetic resonance imaging study.J Neurol Sci. 2019 Dec 15;407:116546. doi: 10.1016/j.jns.2019.116546. Epub 2019 Oct 19. J Neurol Sci. 2019. PMID: 31669731
-
Sixth Nerve Palsy from Cholesterol Granuloma of the Petrous Apex.Front Neurol. 2017 Feb 15;8:48. doi: 10.3389/fneur.2017.00048. eCollection 2017. Front Neurol. 2017. PMID: 28261154 Free PMC article.
-
Isolated unilateral sixth nerve palsy in a patient with nasopharyngeal carcinoma.Rom J Ophthalmol. 2019 Oct-Dec;63(4):375-378. Rom J Ophthalmol. 2019. PMID: 31915737 Free PMC article.
-
Cavernous sinus apoplexy presenting isolated sixth cranial nerve palsy: case report.Pituitary. 2012 Dec;15 Suppl 1:S37-40. doi: 10.1007/s11102-011-0312-5. Pituitary. 2012. PMID: 21503686 Review.
-
Isolated sixth nerve palsy: an uncommon presenting sign of multiple sclerosis.J Neurol. 2000 Sep;247(9):701-4. doi: 10.1007/s004150070114. J Neurol. 2000. PMID: 11081810 Review.
Cited by
-
External auditory canal involvement by nasopharyngeal carcinoma via eustachian tube spread: A case report.Radiol Case Rep. 2024 Aug 7;19(10):4604-4609. doi: 10.1016/j.radcr.2024.07.077. eCollection 2024 Oct. Radiol Case Rep. 2024. PMID: 39220784 Free PMC article.
-
Isolated sixth nerve palsy: a rare first presentation in multiple sclerosis.BMJ Case Rep. 2022 May 11;15(5):e247928. doi: 10.1136/bcr-2021-247928. BMJ Case Rep. 2022. PMID: 35545312 Free PMC article.
-
Effects of CIK Cell Therapy Combined with Camrelizumab on the Quality of Life in Patients with Nasopharyngeal Carcinoma and Analysis of Prognostic Factors.Comput Intell Neurosci. 2022 May 9;2022:5655009. doi: 10.1155/2022/5655009. eCollection 2022. Comput Intell Neurosci. 2022. Retraction in: Comput Intell Neurosci. 2022 Dec 26;2022:9854614. doi: 10.1155/2022/9854614. PMID: 35586106 Free PMC article. Retracted.
References
-
- Devi BC, Pisani P, Tang TS, Parkin DM. High incidence of nasopharyngeal carcinoma in native people of Sarawak, Borneo Island. Cancer Epidemiol Biomarkers Prev. 2004;13(3):482–486. - PubMed
-
- Khuhaprema T, Srivatanakul P, Attsara A, Sriplung H, Wiangnon H, Sumitsawan Y. Nasopharyngeal carcinoma. Cancer Thail. 2010;21:vii308.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
