

Is the clinical manifestation of anaphylaxis in children influenced by the trigger of reaction?
- PMID: 34849125
- PMCID: PMC8610057
- DOI: 10.5114/ada.2020.95650
Is the clinical manifestation of anaphylaxis in children influenced by the trigger of reaction?
Abstract
Introduction: The number of anaphylaxis diagnoses in children is rising, being still based on the clinical picture.
Aim: To determine whether triggers of anaphylaxis influence its clinical characteristics in children and adolescents.
Material and methods: The study group included 114 children (5 months-17 years, mean age: 8.0 ±4.8 years), (66%: boys) with the episode of anaphylaxis up to 1 year back. Medical data were entered to the NORA Registry by means of a validated structured on-line questionnaire.
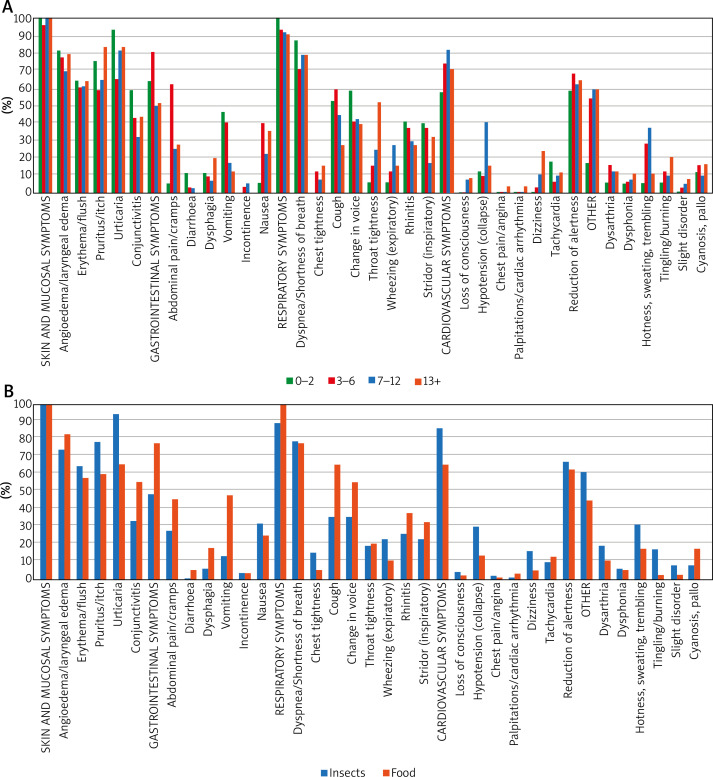
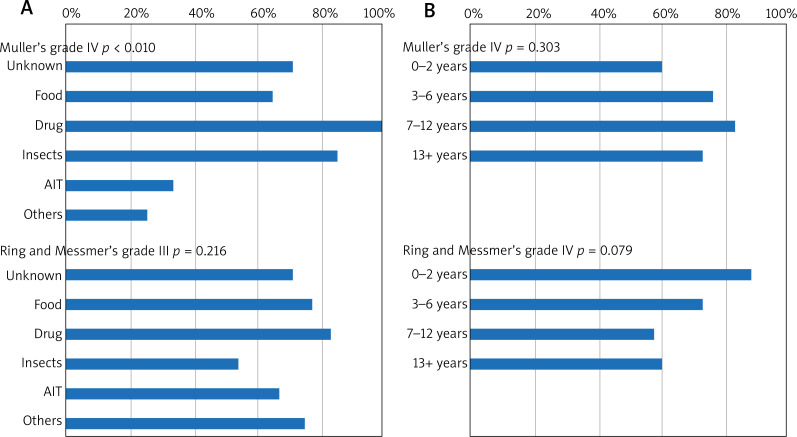
Results: Three most frequent triggers of anaphylaxis were: insect venom (47.4%), food (35.1%), drugs (5.3%), with a predominance of food (egg white, cow's milk, nuts and peanuts) in the 0-6 years age group, while insect venom (bee predominance) in the 7-17 years age group (p = 0.016). Clinical manifestations differed between food vs. venom allergic reactions and presented as gastro-intestinal (GI) (61.4%) (p = 0.004), respiratory (RS) (93.9%) (p = 0.036), and cardiovascular (CVS) (74.6%) (p = 0.022) symptoms. Among objective symptoms, vomiting was the most common symptom in the 0-2 years age group (47.1%) (p = 0.006), while hypotension in those aged 7-12 years (40%) (p = 0.010). Severity of symptoms evaluated as Mueller's grade (IV - 74.5%) and as Ring and Messmer's grade (III - 65.8%), depended on the trigger (p = 0.028, p = 0.029, respectively). Life-threatening symptoms occurred in 26 children (fall of the blood pressure - 22%, loss of consciousness - 4.4%).
Conclusions: The clinical manifestation of anaphylaxis in children is both trigger and age dependent, irrespective of the gender. A typical patient with food anaphylaxis was younger, presenting predominantly GI symptoms, while a typical patient with venom anaphylaxis was older, with mostly cardiovascular symptoms.
Keywords: anaphylaxis; children; clinical manifestation; trigger of anaphylaxis.
Copyright: © 2021 Termedia Sp. z o. o.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Goetz VL, Kim K, Stang AS. Pediatric anaphylaxis in the emergency department: clinical presentation, quality of care, and reliability of consensus criteria. Pediatr Emerg Care. 2019;35:28–31. - PubMed
-
- Biló BM, Rueff F, Mosbech H, et al. EAACI Interest Group on Insect Venom Hypersensitivity Diagnosis of Hymenoptera venom allergy. Allergy. 2005;60:1339–49. - PubMed
-
- Sampson HA. Anaphylaxis and emergency treatment. Pediatrics. 2003;111:1601–8. - PubMed
LinkOut - more resources
Full Text Sources